Download
1 / 44
460 likes | 742 Vues
IN THE NAME OF GOD THYROID DISORDERS & PREGNANCY by ELHAM FAGHIHIMANI ENDOCRINOLOGIST. THYROID PHYSIOLOGY IN NORMAL PREGNANCY.

E N D
IN THE NAME OF GOD THYROID DISORDERS & PREGNANCY by ELHAM FAGHIHIMANI ENDOCRINOLOGIST
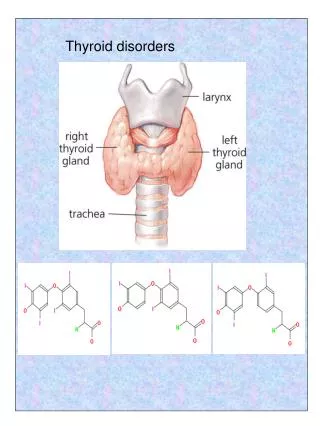
THYROID PHYSIOLOGY IN NORMAL PREGNANCY In women with normal thyroid function there is an increase in thyroxine (T4) and triiodothyronine (T3) production, which results in inhibition of thyroid-stimulating hormone (TSH) in the first trimester of pregnancy, due to a high human chorionic gonadotropin (hCG) level that stimulates the TSH receptor.
Why higher thyroxine requirements in pregnancy? • A large plasma volume and thus an altered distribution of thyroid hormone • increased thyroid hormone metabolism, • increased renal clearance of iodide, • higher levels of hepatic production of thyroxine-binding globulin (TBG) in the hyperestrogenic state
Although the fetal thyroid in humans is histologically developed and can synthesize thyroid hormone by the 10th to 12th week of gestation, thyroid maturation takes longer, and it is not until midgestation that substantial amounts of thyroid hormone are produced by the fetal thyroid gland. Maternal hypothyroidism during the first trimester can thus have deleterious effects on fetal neurodevelopment, which is largely dependent on maternal thyroxine.
Epidemiologic and prospective evidence suggests that early-gestation maternal hypothyroidism can result in mental and motor delay in children when assessed at 1 and 2 years of age, and in some cases may even lead to profound mental retardation and cretinism
The National Health and Nutrition Examination Survey (NHANES 1999–2002) indicates that 3.1% of women of reproductive age in the United States may have hypothyroidism. The prevalence of overt hypothyroidism in pregnancy is estimated to be between 0.3% and 1.5% in different studies
The most common cause of maternal hypothyroidism worldwide is iodine deficiency, but in developed countries autoimmune thyroid disease or Hashimoto’s thyroiditisis more prevalent. The WHO recommends that pregnant and lactating women have an iodine intake of 250 mg per day, which is 100 mg above that recommended for nonpregnant adults, to compensate for increased thyroxine requirements, renal iodine losses, and fetal iodine requirements in pregnancy
Some studies • Thyroid autoimmunity is an important marker for subsequent development of hypothyroidism • The measurement of antibody levels may be helpful in determining the frequency of monitoring thyroid function during the remainder of gestation.
when euthyroid pregnant women with TPO-Abpositivity were treated with levothyroxine (low dose 0.5–1.0 mg/kg/d) to normalize serum TSH, the rate of miscarriage was similar to antibody negative women (3.5% vs 2.4%), whereas untreated TPO-Ab–positive pregnant women had a significantly higher TSH and a higher miscarriage rate of 13.8%.
A TSH level above 6 mU/mLwas associated with a fourfold increase in fetal death in one population-based study of more than 9000 pregnant women. • A large cohort of TPO-Ab–negative pregnant women showed that those with a TSH of 2.5 mU/mL or less in the first trimester had a lower rate of spontaneous pregnancy loss (3.6%) than women with a TSH between 2.5 and 5 mU/mL (6.1%).
A cohort of more than 17,000 women found that pregnancy in those with subclinical hypothyroidism was 3 times more likely to be complicated by placental abruption and had twice the risk of preterm delivery. • The rate of miscarriage was 17% in women with positive thyroid antibodies compared with 8.4% in autoantibody-negative women.
This observation suggests that the upper limit of normal for TSH in the first trimester of pregnancy should be 2.5 mU/mL.
Screening for thyroid disease in pregnancy • The Endocrine Society recommend targeted case- finding in pregnant women with: • a personal history of thyroid disease, • a positive family history, • type 1 diabetes mellitus or other autoimmune disorders • infertility • history of miscarriage or preterm delivery • clinical signs or symptoms of thyroid disease that would classify them as high risk. • up to one-third of hypothyroid women (TSH >4.2 mU/mL) will be missed with case-finding alone
in women with a prior history of hypothyroidism the preconception and first-trimester TSH level should not exceed 2.5mU/mL. In the second and third trimesters, a TSH of less than 3.0mU/mL is desirable. A pregnant woman receiving an established, stable dose of levothyroxine will likely need a 30% to 50% dose augmentation by the fourth through sixth week of gestation
ATA recommendation The goal of LT4 treatment is to normalize maternal serum TSH values within the trimester-specific pregnancy reference range (first trimester, 0.1–2.5mIU/L; second trimester, 0.2–3.0mIU/L; third trimester, 0.3–3.0mIU/L). 4 hours interval between Ca and Fe intake and levothyroxin
Euthyroid women with TPO-Abs are believed to be at high risk for developing hypothyroidism later in pregnancy, and should be monitored for TSH elevation and receive prenatal counseling; however, treatment with thyroid hormone is not yet recommended in this population
Monitoring of thyroid function tests in pregnant women with hypothyroidism should occur frequently, as often as every 2 to 4 weeks throughout midgestation and 4 to 8 weeks in the second half of pregnancy, as this time interval has been shown to identify 90% of abnormal TSH values that resulted in Levothyroxine dose adjustment.
HYPERTHYROIDISM The differential diagnosis of thyrotoxicosis in pregnancy is similar to that of nonpregnant women: autoimmune thyroid disease(eg, Graves’ disease, hashitoxicosis), toxic adenoma or goiter, transient thyroiditis (eg, subacutethyroiditis, silent thyroiditis), iodine-induced hyperthyroidism and, rarely, a pituitary adenoma secreting TSH or thyroid hormone resistance
Additional consideration of hCG-mediated hyperthyroidism including gestational transient thyrotoxicosis(GTT) and its association with hyperemesisgravidarumbecomes very important. • Postpartum thyroiditisis also unique to the pregnant cohort within several months of delivery.
The most common cause of hyperthyroidism in pregnancy, as in all women of reproductive age, is autoimmune Graves’ disease with circulating TSH receptor antibodies (TRAbs) stimulating the thyroid gland and TSH receptor. Graves’ disease may be challenging to diagnose in the hypermetabolic state of pregnancy because of similar symptoms in both conditions.
Features suggestive of Graves’ hyperthyroidism in normal pregnancy include: a diffuse goiter, evidence of ophthalmopathy, TRAb or thyroid-stimulating immunoglobulin (TSI) positivity, and a family history of autoimmune thyroid disease. The extent of elevation of thyroid function tests typically is higher in Graves’ disease than in hyperemesisgravidarum. The immune-tolerant state of pregnancy is associated over time with a decrease in TRAb titers, thus the hyperthyroidism secondary to Graves’ disease may subside in severity as gestation progresses
Gestational Transient Thyrotoxicosis GTT differs from Graves’ disease in that it is a self-limited, nonautoimmuneform of hyperthyroidism with negative TRAbs. it is related to the elevation of hCG, which can then cross-react with the TSH receptor and induce thyroidal iodothyronine secretion
Gestational Transient Thyrotoxicosis Women have a TSH in the low to normal range for pregnancy or is frequently undetectable, elevated free T4 and free T3 levels, and prolonged abnormally high hCGin the first and second trimesters, occasionally higher than 100,000 U/L. These patients present with symptoms of hyperthyroidism in about 50% of cases, and the emesis or symptoms from thyrotoxicosis may be severe enough to require hospitalization.
Hyperemesisgravidarum characterized by excessive nausea and vomiting, which causes a greater than 5% weight loss, dehydration, and ketonuria in early pregnancy, is a milder form of GTT in that women have subclinical or very mild overt hyperthyroidism in one-third to two-thirds of cases.
pregnant women with uncontrolled hyperthyroidism: • Preeclampsia, • congestive heart failure, • placental abruption and • cesarean delivery, • thyrotoxic periodic paralysis.
Fetal risks of maternal thyrotoxicosis include: • spontaneous abortion, • premature labor and • low birth weight, • stillbirth, • congenital abnormalities
TREATMENT During pregnancy, medical treatment is preferred despite class D classification of thionamides by the (FDA), because radioactive iodine cannot be used and surgery is typically reserved for severe thyrotoxicosis that has failed medical therapy. PTU had been the drug of choice during pregnancy to avoid MMI-associated scalp defects of aplasia cutis or choanal/esophageal atresia.
Updated guidelines from the ATA and American Association of Clinical Endocrinologists are expected in 2011 to delineate a limited therapeutic window for PTU during the first trimester of pregnancy, in the treatment of thyroid storm, and in patients with minor reactions to MMI who refuse radioactive iodine therapy or surgery; otherwise MMI should be used in every patient who chooses antithyroid drug therapy for Graves’ disease
The goal of therapy is to use the lowest dose of medication to maintain maternal free T4 in the upper nonpregnant reference range, as this minimizes the risk of hypothyroidism to the fetus.
radioactive iodine administration for diagnostic scans and treatment is absolutely contraindicated in pregnant patients and in women considering becoming pregnant in the near future, secondary to adverse effects on the fetus and the fetal thyroid gland.
Thyrotoxicosis and primary hyperthyroidism in the neonate is usually transient, and remits with clearance of maternal TRAbs in the first 3 to 6 months of life. postpartum short-term levothyroxine administration to the hypothyroid neonate is recommended, and the hyperthyroidism should only be treated with antithyroid agents if the neonate has clinically severe thyrotoxicosis.
When the mother is euthyroid after treatment of Graves’ disease, is at risk of recurrence, especially postpartum, and her thyroid function should be monitored during pregnancy and after delivery. If the mother has had thyroid ablation or surgery she may still be TRAb positive, and antibodies may cause fetal hyperthyroidism via passage through the placenta.
TRAb titers should be measured before pregnancy or at the end of the second trimester in all pregnant women with current or a history of Graves’ disease to assess the risk of neonatal hyperthyroidism in the fetus. If titers are high, fetal ultrasonography is necessary to look for growth restriction, hydrops, goiter, and cardiac failure in addition to clinical monitoring of the fetus for hyperthyroidism
Subtotal thyroidectomycan usually be performed in the second trimester of pregnancy, in situations whereby: • Hyperthyroidism is uncontrolled with ATDs • Treatment requires persistently high doses of antithyroid medication (generally thought to be more than approximately 300 mg of PTU daily) • If the mother has a serious adverse effect to medical therapy.
Women who receive I-131 therapy for Graves’ disease should wait at least 6 months before becoming pregnant, although this is an empiric recommendation. These patients should become hypothyroid within 2 to 3 months, and it may subsequently take 1 to 2 months to restore euthyroidism with exogenous levothyroxine.
Lactation and Treatment of Thyroid Dysfunction Breastfeeding is considered safe in mothers with hypothyroidism and hyperthyroidism taking thyroid medications. Although MMI and PTU both appear in human milk, it is at very small concentrations The decision whether to breastfeed while taking antithyroid agents is an individual decision that should be discussed by the patient and her physician.
Postpartum Thyroid Dysfunction an autoimmune destructive thyroiditis (PPT) with a period of thyrotoxicosis, hypothyroidism, or both, followed by recovery in the first year after delivery. It is frequent and occurs in about 8% of women worldwide, and is strongly associated with TPO-Ab positivity. PPTD occurs most frequently at about the fourth month after delivery, although it can take place any time between 1 and 12 months postpartum.
Up to 50% of pregnant women with TPO-Abs will develop PPTD, and of these about 20% may develop permanent hypothyroidism over the next several years. Risk factors for subsequent and permanent hypothyroidism include a postpartum peak TSH greater than 20 mU/mL, a high titer of TPO-Abs, hypoechogenicity on thyroid ultrasonography, and a hypothyroid phase of PPTD.
The hypothyroid phase of PPTD should be considered for treatment with levothyroxine at replacement doses, especially when TSH is 10 mU/mLor greater. stop the medication after approximately 6 to 12 months of treatment to determine if the hypothyroidism is permanent and then, if normal, perform periodic monitoring.
The Endocrine Society recommends screening for PPTD by measuring TSH at 3 and 6 months postpartum in all women with TPO-Abs and type 1 diabetes mellitus, as well as annually in those with a history of PPTD in prior pregnancy. Mothers who experience depression in the postpartum period should also be screened for hypothyroidism, and treated accordingly.