Download
1 / 32
320 likes | 436 Vues
Reduction of Medicaid Expenditures from State Prescription Programs in Illinois and Wisconsin. Donald S Shepard, PhD* Desiree Koh, * Cindy Thomas, PhD* Grant Ritter, PhD* Daniel Gilden,+ William Stason, MD,MS* Christine Bishop, PhD* *Brandeis University; +JEN Associates

E N D
Reduction of Medicaid Expenditures from State Prescription Programs in Illinois and Wisconsin Donald S Shepard, PhD* Desiree Koh, * Cindy Thomas, PhD* Grant Ritter, PhD* Daniel Gilden,+ William Stason, MD,MS* Christine Bishop, PhD* *Brandeis University; +JEN Associates Supported by the Centers for Medicare & Medicaid Services under Contract No. CMS 500-00-0031/T.O. #2 to Brandeis University AcademyHealth Annual Research Meeting, June 8-10, 2008
Framework Better use of drugs and medical services Prescription coverage Less Medicaid entry Maintain health Lower nursing home use
Past research • Rector (2004), Safran (2005), Leung (2005) – About 30% of low income people skip some prescribed medications • Soumerai et al. (1991) –Limiting drugs to vulnerable population increased nursing home admissions • Gilman (2004) – Members of Prescription Assistance Programs (PAP) skip fewer doses than comparable controls • Shepard (2006) – SeniorCare halved risk of skimping • Leung (2005) – Risk is related to individual characteristics
In mid-2002, Illinois and Wisconsin initiated “SeniorCare” (SC) pharmacy assistance programs (PAPs) that provide low-income persons aged 65+ with publicly funded prescription drug assistance. Maximum co-payments per prescription are generally $4 in IL and $15 in WI. Enrollees with incomes up to 200% of the federal poverty limit (FPL) are funded under a Medicaid waiver designed to help seniors improve prescription drug use, maintain health and reduce financial vulnerability due to prescription costs. Program background
68,292 Wisconsin members, who were all new enrollees (1,189 interviewed), 121,000 Illinois members previously in Circuit Breaker, a limited PAP that excluded mental health and gastro-intestinal drugs and automatically rolled over into SC (termed ‘IL rollovers, 374 interviewed); 47,782 Illinois members not previously in this PAP (termed ‘IL new,’ 664 interviewed). Three strata studied
Study Design for Medicaid Analysis • Ohio served as the comparison state. • Using Medicare claims and zip codes, matched Illinois and Wisconsin enrollees exactly on demographic and disease categories to similar Ohio Medicare beneficiaries. • Used propensity scores to match closely on disease severity and socio-economic characteristics based on census information and Social Security benefits.
Population Studied • Needed precise matching on income for examining Medicaid entry • Limited this analysis to buy-in Medicare beneficiaries in the three states • Received subsidies for Medicare premiums and deductibles • Qualified Medicare Beneficiaries, QMB • Special Low Income Medicare Beneficiaries, SLMB • We matched 7,699 Illinois and 1,798 Wisconsin buy-in beneficiaries to comparable buy-in Ohio controls.
Research Objective:Evaluate First Year Impacts on • Nursing home entry • Medicaid entry • Medicaid expenditures
Approach • Descriptive analysis • Multivariate analysis
Nursing Home Entry among Wisconsin Buy-in Beneficiaries and Matched Ohio Controls
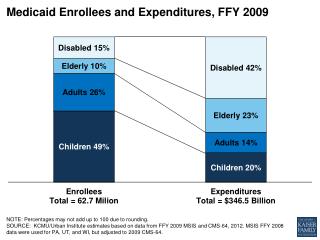
Medicaid Entry amongWisconsin Buy-in Beneficiaries and Matched Ohio Controls
Illinois summary • Due to preexisting PAP, SeniorCare did not reduce Medicaid entry, but did reduce nursing home entry and spending. • Cumulative rate of nursing home entry of Illinois SeniorCare buy-in beneficiaries (2.4%) was half the rate of the matched Ohio controls (4.4%). • Medicaid spending over the first year when averaged over all Illinois buy-in SeniorCare members (with standard errors of the mean) was $631 ($26) vs. $1,605 ($83) for matched buy-in Ohio controls • Per enrollee savings $974 ($87) or 61%. • Savings in Illinois did not quite equal the state’s share of first-year program costs per enrollee year ($1,394).
Wisconsin summary • SeniorCare buy-in enrollees had half the rate Medicaid entry in the first year (11%) than matched Ohio controls (22%) • Wisconsin SC had half the rate of nursing home entry (2.2%) compared to Ohio controls (4.5%) • Had $1,190 ($163) or 81% lower Medicaid spending per buy-in enrollee. • Wisconsin savings on buy-ins were greater than the state’s share of first-year program costs per enrollee year ($1,032).
Extrapolation possible? • Question: Do the data allow examining impacts on nursing home and Medicaid for all SeniorCare enrollees? • Answer: No • Why not? Ascertainment of income
Conclusions • 50% reductions in skimping applied to all SeniorCare enrollees • Comparable declines in nursing home entry among buy-ins. • First year savings in buy-in population not quite enough to pay for the program costs in Illinois • These savings were more than sufficient in Wisconsin. • Prescription drug coverage for vulnerable populations pays off with less nursing home entry and lower costs.
Limitations • Differences in nursing home and Medicaid policies among states could confound interpretation
Strength: Consistent improvements in • Self reported behavior (skimping) • Costly services (nursing home entry) • Medicaid expenditures
Research implications • Observations and natural experiments very powerful. • Must understand and control for selection effects. • Stay within the data.
Policy implications • Enrollment of needy elders in both states benefited from outreach, straightforward design, and federal subsidies that extended to 200% of the FPL. • These findings show the value of completing “coverage” with access to prescription drugs.
Thank you Shepard@brandeis.edu