Download
1 / 29
290 likes | 317 Vues
Guidelines for managing a 34-year-old unresponsive female with prior bariatric surgery, covering patient history, symptoms, pre-hospital concerns, and discharge recommendations. |

E N D
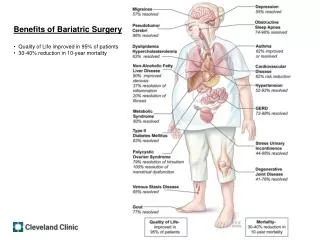
Acute Management of Patients with a Prior History of Bariatric Surgery
Bariatric Surgery Types • Gastric Bypass • Sleeve Gastrectomy • Lap-Band—rarely performed now • VBG (Gastric Stapling)—obsolete • Molina Band—obsolete • Other: (Duodenal Switch, BPD)—rare
Overview • Obtaining patient history • Symptoms related to the bariatric surgery • Procedure concerns • Medication contraindications • Tobacco/Alcohol Use • When to notify the bariatric surgeon • Discharge recommendations
Pre-Hospital Concerns • Successful bariatric patients are difficult to identify • Bariatric GI changes can affect field medications and procedures • Symptoms may be directly related to the bariatric procedure regardless of surgical date.
Patient History • Reasons the patient will not disclose a history of bariatric surgery: a. Does not feel the need to disclose if the current problem appears unrelated b. Shame related to weight regain or non- compliance c. Secrecy from family and friends
Bariatric History Information • Specific type of weight loss procedure • Date of surgery with location and surgeon’s name if available • Any history of complications • Description of follow-up compliance • Exact medication history including OTC’s • Social history with tobacco and alcohol usage
History Helpful Tips • Try to obtain sensitive history information while alone with the patient • Suspect bariatric surgery if there is/was a history of morbid obesity • Ask specific questions about stomach surgery even when the current problem is not related • Ask all bariatric patients specifically about NSAID (Rx & OTC) and tobacco use • Educate the patient how this information is needed to avoid complications related to medications or procedures
Common Symptoms • Abdominal Pain • Chest Pain • Nausea/Vomiting • GI Bleeding • Weakness • Shortness of Breath • Bloating • Illness/Injury unrelated to bariatric anatomy
Abdominal Pain • Epigastric: Gastritis/Ulcer disease is most likely—think food obstructing the gastric bypass pouch, lapband, or stomach sleeve when the pain is associated with vomiting • Right Upper Quadrant: Gallbladder disease occurs more often with rapid weight loss • Generalized: Internal intestinal hernias often present with vague pain only • Lower Quadrants: Constipation or conditions unrelated to bariatric changes, i.e. appendicitis
Abdominal Pain Considerations • The type of bariatric surgery will often dictate the evaluation and treatment • Gastric bypass patients with common bile duct stones cannot be treated with a traditional ERCP • Bariatric patients with bowel obstructions may present with pain and bloating without vomiting
Chest Pain • Bariatric patients with stomach ulcers often present with chest pain as the only symptom • Food obstructions cause esophageal dilation and spasm, resulting in chest pain • Must rule out cardiopulmonary etiologies
Nausea/Vomiting • Common symptom in bariatric patients <30 days post-op • The most common symptom in Lapband patients • Most often originates from a problem in the stomach
GI Bleeding • Upper and lower GI bleeding can occur in bariatric patients • Gastric bypass patients with bleeding ulcers often pass bright red blood due to the rapid transit time
Weakness • Often a symptom of dehydration • May be the presenting symptom in gastric bypass patients with a thiamine deficiency associated with vomiting or alcohol use • Consider malnourishment in bariatric patients • B-12 deficiency can cause weakness when prolonged—B-12 replacement is needed in all gastric restrictive patients due to the loss of intrinsic factor
Shortness of Breath • Post-surgical gastric leaks will present with symptoms very similar to pulmonary embolus or congestive heart failure • A leak should be considered in any bariatric patient with shortness of breath < 30 days post-op
Bloating • Bariatric surgery can change the GI tract anatomy, which prevents vomiting with bowel obstructions • Bloating and abdominal pain may be the only symptoms with intestinal twisting (volvulus) or blockage
Unrelated Illness/Injury • Many ER/Hospital admissions are not related to the prior bariatric surgery • An accurate history of any bariatric procedure is needed to avoid potential injury to the stomach with procedures or medications • The bariatric history will be needed to order an appropriate diet
Procedure Concerns • All bariatric procedures either create a narrow opening into the stomach or restrict the total size of the stomach • Misplacement and injury to the GI tract are the two most common problems with blind advancement of tubes • Gastric tubes will rarely pass blindly through an inflated Lapband, resulting in the tube curling in the esophagus
Procedure Concerns • Blind placement of tubes in gastric bypass patients will usually result in the tube abruptly stopping at the wall of the small intestine adjacent to the stomach pouch increasing the possibility of intestinal perforation • Drug overdose--blind gastric lavage of bariatric patients is contraindicated
Procedure Concerns • Gastric bypass patients with biliary common duct stones cannot be treated with a traditional ERCP • Oral contrasted studies of the stomach need to be modified to account for the small gastric size
Medication Contraindications • All Cox-1 NSAIDS, both Rx and OTC, including injectables are an absolute contraindication in gastric bypass patients due to the high incidence of marginal ulceration • Full strength aspirin medications and oral corticosteroids should be used with caution due to the potential erosive properties
Tobacco/Alcohol Use • Smoking tobacco causes ischemic erosions in gastric bypass patients. • Alcohol use/abuse on a routine basis increases the likelihood of gastritis and ulcers in patients with restricted stomach volume
*****Bleeding/Perforated Ulcers in Gastric Bypass Patients are most often related to smoking tobacco or NSAID use*****
When to notify the bariatric surgeon • All bariatric patients presenting to the ER less than 30 days after bariatric surgery • Any bariatric patient greater than 30 days post-operative presented with a bariatric-related complaint, including chest pain, abdominal pain and weakness • Any Lapband patient with vomiting • Any time there are concerns or questions involving the bariatric anatomy
Discharge Recommendations • Follow up suggested for all bariatric patients seen in the ER less than 30 days post-operative • Follow up with the bariatric clinic if the patient has not been compliant with visits • Urge the patient to stop NSAIDS and tobacco when use is detected in bariatric patients
Test Question • NSAIDS (Cox-1) are contraindicated in gastric bypass patients, regardless of an oral or intra-venous route a. True b. False
Test Question • Bariatric patients often do not reveal a history of weight loss surgery because: a. They never told family and/or friends about the bariatric surgery b. They are ashamed about inadequate weight loss c. They believe it is not necessary to reveal when presenting with an unrelated problem d. All of the above
Test Question • The bariatric surgeon should be notified if a Lapband patient presents with persistent vomiting a. True b. False