Download
1 / 32
320 likes | 436 Vues
HIV/AIDS epidemiology and prevention policy in Finland. Mika Salminen Kansanterveyslaitos – KTL National Public Health Institute. Country Profile.

E N D
HIV/AIDS epidemiology and prevention policy in Finland Mika Salminen Kansanterveyslaitos – KTL National Public Health Institute
Country Profile • HIV-infection and AIDS are reportable diseases in Finland. Neither condition is classifi ed as a generally dangerous disease, which excludes the use of any compulsory measures in prevention or control. • By law, both diagnostic laboratories and physicians report cases to the Finnish National Public Health Institute (KTL), which maintains the National Infectious Disease Registry (NIDR) for passive surveillance purposes. • Voluntary targeted unlinked-anonymous studies are used to address prevalence in vulnerable groups. • Blood donations are universally screened for HIV and all pregnant mothers are offered HIV testing (opt-out regimen in place since 1997).
Prevalence and Incidence • General population prevalence and incidence of HIV and AIDS are low in Finland. • HIV prevalence rate of approximately 2 / 10,000 population* • HIV incidence rate of approximately 37 / million population* • HIV prevalence among vulnerable groups is higher: • Estimated HIV prevalence among MSM: 4.5% (2.6–7.3%, CI 95%) ** • Estimated HIV prevalence among IDU: 1.4% (0.5–3.2%, CI 95%) ** based on passive surveillance data (2006) ** based on cross sectionasectional unlinked-anonymous sampling data (2006 and 2005)
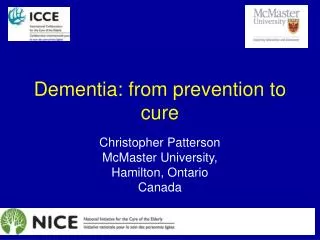
Flow of data and information in the national infectious disease register (NIDR), 1995 -
Main objectives of the HIV/AIDS prevention policy • Prevention of new infections is the key target of policy measures. For those who become infected, there is guaranteed free access to medically indicated treatment and care. • Support for full social empowerment of persons who have been infected to reduce their vulnerability is an essential part of prevention policies. • Management of prevention activities through national coordination and a multidisciplinary public/private partnership approach.
Field of HIV prevention Intentional risktaking Risks and ampifying factors Lack of knowledge Marginalisation Lack of understanding Lack of tools Violence and use Of force High prevalence Unprotected sex Mother to child Unsafe blood And tissue products Economic realities (sexwork) Drugs and alcohol
Financial resources for HIV/AIDS prevention • The public financial resources allocated to HIV/AIDS prevention are divided between multiple actors and sectors. • In many cases HIV/AIDS prevention activities are linked to general health prevention and education activities. • There is no specific budget line for the purpose, and a comprehensive estimate of resources used for this purpose has not been made.
Risk perception and awareness • Risk groups as a term give false pretence: ”If I do not belong to a certain group, I’m not at risk” • Risks dependant on risktaking • AIDS/HIV prevention messaging fatigue may over time lead to loss of awareness • Constant struggle to keep up awareness of risks • Safe sex promotion has to be constantly kept up with
1.Prevention of new infections is key • Health education and promotion are the main modes of infuencing the development of the future epidemic • Youth are the most important target group and gay and bisexual groups must also be reached. • Impact trough schools: health education as a subject for pimary level grades 7-9 and secondary level 1-3 • Includes sexual health and STD risks • Prevention of both infection risks and drug use among Injecting drug users are equally important. • Prevention of sexual transmission among youth needs new approaches • Special attention need to be directed to prisons, socially marginalised group, immigrants and sex workers • Prevention of MTCT must be as comprehensive as possible
2. Health service role • A comprehensive health and social service system is an essential part of HIV prevention • For those living in Finland diagnostics, treatment, care and support are all free of charge, including ARV-treatment. Health service access is not tied to employment. • The threshold to seeking AND offering HIV testing must be kept low, but strictly voluntary (excp. Blood & tissue donors). • Anonymous testing outside the established health system fulfils an important role and must be supported.
3. PLWH as equal members of society • Attitudes and knowledge among the general population must not become discriminatory against those living with HIV • Legal measures must be put in place to prevent discrimination in all areas of life, including the health- care services, social and educational services
HIV/AIDS issues built into general legislation • Constitution • Act on the Status and Rights of Patients • Primary Health Care Act • Act on Specialized Medical Care • Personal Data Act and Personal Data File Decree • Communiable Disease Act and associated decree • Act on the Protection of Privacy in Working Life
Constitution • Provides the basic protection against discrimination • Protection against discrimination due to race, gender, sexual orientation, social and health status etc. • > no basis for discrimination in any setting due to HIV infection • > HIV-infected have equal rights to work, healthcare and all other governmental services • HIV-infected can work in all areas of society, also within healthcare services
Primary healthcare • Primary healthcare through municipal health centers • Responsible for preventive and health promotion services • All primary care covered • Access to free of charge voluntary HIV testing and councelling, VCT (subjective right of access regulated by ministerial decree) • No automated screening groups, but testing offered routinely to expecting mothers • Physician initiated most follow VCT • Workers healthcare: parallel system paid by the employers
Specialised Healthcare • Specialised care through hospital district central and university hospitals • Treatment and secondary care • Access to HIV/AIDS treatment and care is free of charge for all legal residents (governed by HIV/AIDS belonging a category of fully covered diseases)
Law and ordinance on personal identity protection • Information on personal identity even within the health care system is strongly protected • Information cannot be shared between different service providers without explicit written consent of the client • Information allowing identification of individuals cannot be shared with other authorities such as the police, insurance companies or even prison services • Within the prison system, healthcare personnel cannot share information on prisoner health status with prison management or guards • Workers healthcare services cannot share information on individual persons with employer
Law and ordinance on Infectious diseases • Governs the classification of infectious diseases into reportable and non reportable categories • Covers control measures available according to individual disease properties • HIV/AIDS reportable, but no force measures applied (in contrast to i.e.Tuberculosis) • Specifies certain responsibilities for the municipal prevention and health promotion services for example for the group of injecting drug users
Law (and ordinance) on Infectious Disease Control 1.1.2004 (free translation from Finnish) • Law on communicable diseases 25.7.1986/583 (with changes 2004) • Ordinance on communicable diseases 31.10.1986/786 • 6 § ....The municipal authority responsible for communicable disease control and as its sunbordinate, the municipal health care physician responsible for communicable diseases, must as a task specified by the Law on Communicable Disease also:1) Organise communicable disease control activities in the municipal health care area, such as communicable disease information distribution, health education and health advice, including health advice services and exchange of injection equipment for injecting drug users as specified by the need for communicable disease control.
IDU health policy implementation • Establisment of a Network of Low Threshold Health Service Centers (LTHSC) for IDU in Finland • Trust-based function: voluntary, not based on beeing drug-free, personal information not recorded • Close and accessible to target group • Services include smallscale healthcare provision, councelling & guidance to detoxification, VCT & HIV-testing, vaccinations (tetanus, HBV, HAV), condom distribution and exchange of injection equipment • Base for outreach work among IDU • Close collaboration with detox- and primary health care services, social services and law enforcement
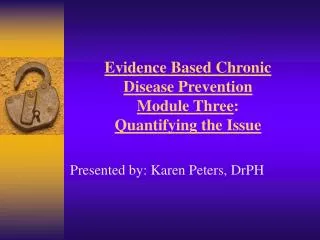
Impact on HIV- and Hepatitis epidemic in Finland Number of LTHSC • LTHSC –network in • Finland • 21 municipalities • > 30 sites • 2004 – statutory • obligation for • municipalities to • provide services, • Including inj.equipment • exchange HIV HCV
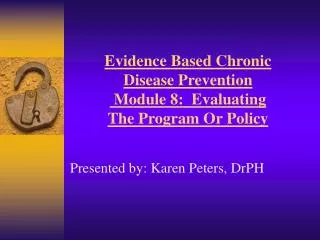
LTHSC services 2000-2006 Injection equipment exchange at LTHSC Other access * Preliminary data