Download
1 / 1
10 likes | 122 Vues
Our experience in providing home self-administered therapy to HAE patients Maria Bova 1 * , Angelica Petraroli 1 , Stefania Loffredo 1 , Maria Concetta Siani 1 and Massimo Triggiani 2

E N D
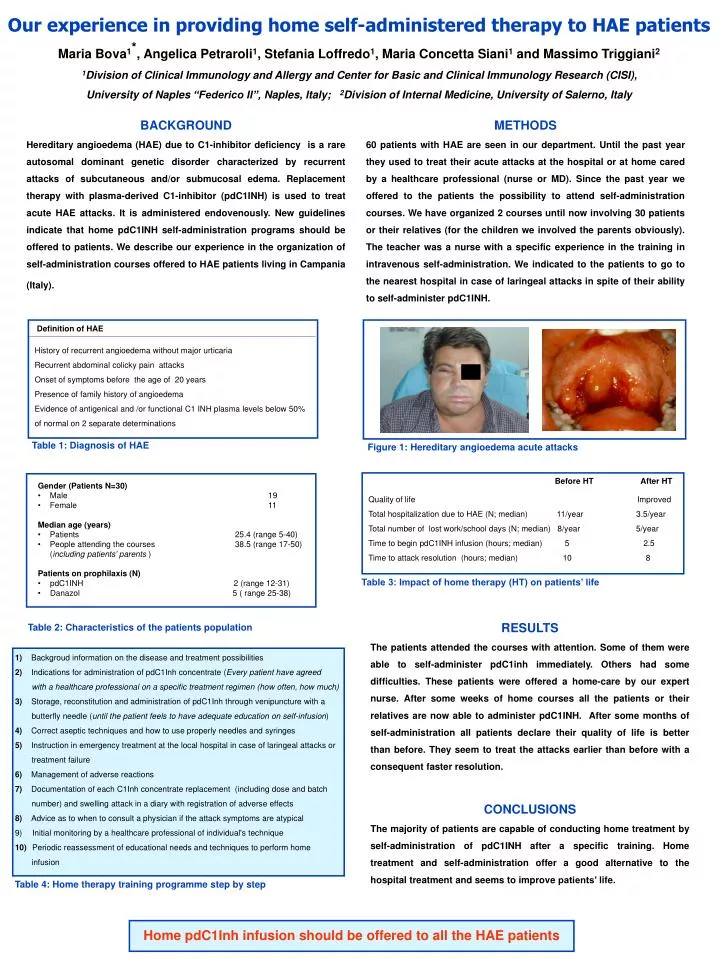
Our experience in providing home self-administered therapy to HAE patients Maria Bova1*, Angelica Petraroli1, Stefania Loffredo1, Maria Concetta Siani1 and Massimo Triggiani2 1Division of Clinical Immunology and Allergy and Center for Basic and Clinical Immunology Research (CISI), University of Naples “Federico II”, Naples, Italy; 2Division of Internal Medicine, University of Salerno, Italy BACKGROUND Hereditary angioedema (HAE) due to C1-inhibitor deficiency is a rare autosomal dominant genetic disorder characterized by recurrent attacks of subcutaneous and/or submucosaledema. Replacement therapy with plasma-derived C1-inhibitor (pdC1INH) is used to treat acute HAE attacks. It is administered endovenously. New guidelines indicate that home pdC1INH self-administration programs should be offered to patients. We describe our experience in the organization of self-administration courses offered to HAE patients living in Campania (Italy). METHODS 60 patients with HAE are seen in our department. Until the past year they used to treat their acute attacks at the hospital or at home cared by a healthcare professional (nurse or MD). Since the past year we offered to the patients the possibility to attend self-administration courses. We have organized 2 courses until now involving 30 patients or their relatives (for the children we involved the parents obviously). The teacher was a nurse with a specific experience in the training in intravenous self-administration. We indicated to the patients to go to the nearest hospital in case of laringeal attacks in spite of their ability to self-administer pdC1INH. Definitionof HAE Historyofrecurrentangioedemawithout major urticaria Recurrentabdominalcolickypainattacks Onsetofsymptomsbefore the ageof 20 years Presenceof family historyofangioedema Evidenceofantigenical and /or functional C1 INH plasma levelsbelow 50% ofnormal on 2 separate determinations Table 1: Diagnosis of HAE • Figure 1: Hereditary angioedema acute attacks Table 3: Impact of home therapy (HT) on patients’ life • 1) Backgroud information on the disease and treatment possibilities • 2) Indicationsforadministrationof pdC1Inh concentrate (Every patient have agreed with a healthcare professional on a specific treatment regimen (how often, how much) • 3) Storage, reconstitution and administrationof pdC1Inh throughvenipuncturewith a butterflyneedle (until the patient feels to have adequate education on self-infusion) • 4) Correctaseptictechniques and howtouseproperlyneedles and syringes • 5) Instruction in emergency treatment at the local hospital in case oflaringealattacks or treatment failure • 6) Management ofadversereactions • 7) Documentationofeach C1Inh concentrate replacement (including dose and batchnumber) and swellingattack in a diarywithregistrationofadverseeffects • 8) Adviceastowhentoconsult a physicianif the attacksymptoms are atypical • Initial monitoring by a healthcare professional of individual's technique • Periodic reassessment of educational needs and techniques to perform home infusion RESULTS The patients attended the courses with attention. Some of them were able to self-administer pdC1inh immediately. Others had some difficulties. These patients were offered a home-care by our expert nurse. After some weeks of home courses all the patients or their relatives are now able to administer pdC1INH. After some months of self-administration all patients declare their quality of life is better than before. They seem to treat the attacks earlier than before with a consequent faster resolution. CONCLUSIONS The majority of patients are capable of conducting home treatment by self-administration of pdC1INH after a specific training. Home treatment and self-administration offer a good alternative to the hospital treatment and seems to improve patients’ life. • Gender (Patients N=30) • Male 19 • Female11 • Medianage (years) • Patients 25.4 (range 5-40) • People attending the courses 38.5 (range 17-50) • (includingpatients’ parents) • Patients on prophilaxis (N) • pdC1INH 2 (range 12-31) • Danazol 5 ( range 25-38) Table 2: Characteristics of the patients population Table 4: Home therapy training programme step by step Before HT After HT Qualityof life Improved Total hospitalization due to HAE (N; median) 11/year 3.5/year Total numberoflost work/schooldays (N; median) 8/year 5/year Timetobegin pdC1INH infusion (hours; median) 5 2.5 Timetoattackresolution (hours; median) 10 8 Home pdC1Inh infusion should be offered to all the HAE patients