
ABSTRACT
Phase I evaluation of sorafenib & bevacizumab as first-line therapy in hepatocellular cancer (HCC) Joleen M. Hubbard 1 , Steven R. Alberts 1 , William S. Loui 2 , Michelle R. Mahoney 1 , Lewis R. Roberts 1 , Thomas C. Smyrk 1 , Zoran Gatalica 3 ,

ABSTRACT
E N D
Presentation Transcript
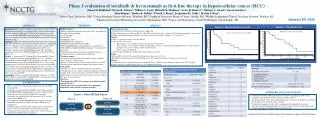
Phase I evaluation of sorafenib & bevacizumab as first-line therapy in hepatocellular cancer (HCC) Joleen M. Hubbard1, Steven R. Alberts1, William S. Loui2, Michelle R. Mahoney1, Lewis R. Roberts1, Thomas C. Smyrk1, Zoran Gatalica3, Shaji Kumar1, Shaker R. Dakhil4, Patrick J. Flynn5, Jacqueline M. Lafky1, Martin J. Bury6 1Mayo Clinic, Rochester, MN; 2Cancer Research Center of Hawaii, Honolulu, HI; 3Creighton University Medical Center, Omaha, NE; 4Wichita Community Clinical Oncology Program, Witchita, KS; 5Minnesota Oncology Hematology Associates, Minneapolis, MN; 6Cancer and Hematology Center W Michigan, Grand Rapids, MI Figure 2. Progression-free survival Figure 3. Overall survival Abstract ID: 4116 Mosaic Chart of LNR & T Stage and AJCC & T Stage Classifications ABSTRACT METHODS RESULTS • Patient Characteristics: • 17 patients were enrolled in the phase I portion of this study • Patient Characteristics are shown in Table 2. The median age was 66 years. 2 patients (12%) had prior radiation, 1 patient (6%) had prior chemoembolization, 3 patients (18%) had vascular invasion, and 12 patients (71%) had ascites • Toxicity: • Grade 3 or 4 adverse events are listed in Table 3. • Cycle 1 DLTs by dose level: • Dose 0 (2 pts) – Gr 3 hand/foot skin reaction, fatigue, hypertension • Dose -1 (3 pts) – Gr 3 alanine/aspartate aminotransferase increase, dehydration, hypophosphatemia, creatinine increase, hypoglycemia, nausea vomiting, and Gr 4 hyponatremia • Dose -2 and -2a had 0 DLTs. • 1 patient death within the first month felt possibly related to treatment • Dosing: • After no DLTs at level -2, the dose of bevacizumab was increased (level -2a) • The MTD was determined to be sorafenib 200 mg twice daily and bevacizumab 2.5 mg/kg every other week • Efficacy: • 16 patients had at least one post-baseline assessment of disease. There were no complete responses, one (6.25%) partial response, 10 (62.5%) stable disease, and 5 (31.25%) progressive disease Background: HCC tumors are highly vascular and over express VEGF. The monoclonal antibody bevacizumab (BEV) and the oral multi-kinase inhibitor sorafenib (SOR) inhibit VEGF-induced angiogenesis and the associated Ras/Raf/MEK/ERK signaling pathway. It is hypothesized that SOR will complement the mode of action of BEV by more fully blocking VEGF signaling. Methods: Eligibility included measurable locally advanced or metastatic HCC not amenable for surgery or liver transplant (BCLC-C), Child Pugh A or B7, esophageal varices if treated ≥ 6 mos, and acceptable blood chemistries. Patients with mixed cholangiocarcinoma/HCC were ineligible. Treatment doses/schedule appears in the table. The phase I starting dose level (0) was: BEV 1.25 mg/kg d1&15 plus SOR 400 mg BID d1-28. Results: 17 patients aged 18-79 (mean 66 yrs) were enrolled; 14 were male. A majority of patients presented with ascites (71%). Baseline characteristics included cirrhosis (41% of patients), prior RT (12%), prior chemoembolization (6%), and vascular invasion (18%). Cycle 1 dose limiting toxicities (DLTs) by dose level were: Dose 0 (2 pts with DLTs) – Gr 3 hand/foot skin reaction, fatigue, hypertension; Dose -1 (3 pts) – Gr 3 alanine/aspartate aminotransferase inc, dehydration, hypophosphatemia, creatinine inc, hypoglycemia, nausea vomiting, and Gr 4 hyponatremia; Dose -2 and -2a had 0 DLTs. Conclusions: With an acceptable toxicity profile, dose level -2a (SOR 200 mg BID d1-28, plus BEV 2.5 mg/kg d1&15) is currently used in the on-going phase II trial in this population. • Eligibity criteria: • Patients with locally advanced or metastatic HCC not candidates for surgery or liver transplant • ≥18 years of age • ECOG PS 0,1 • Child Pugh A or B7 • Standard laboratory parameters • No prior systemic chemotherapy for HCC • Prior chemoembolization, radioembolization, radiofrequency ablation (RFA), or other local ablative therapies ≥6 weeks prior to registration • Evaluation and treatment of known or clinically suspected esophageal varices ≤6 months prior to registration • Treatment regimen: • Sorafenib (continuously per dose schedule) and bevacizumab every 2 weeks on a 28 day cycle • Disease assessments occurred after 4 weeks, then every 8 weeks • Treatment given until PD, unacceptable AE or patient refusal • Study design: • Standard 3 + 3 dose escalation/descalation design (Table 1) • DLT defined as an AE ≥ grade 3 attributed (definitely, probably or possibly) to the study treatment based on NCI CTCAE v3.0 criteria • MTD defined as the dose level below the lowest dose that induces DLT in at least 1/3 of patients • Objectives: • To determine the MTD of bevacizumab in combination with sorafenib for HCC • To determine safety and tolerability of bevacizumab in combination with sorafenib in patients with HCC METHODS Figure 1. Phase I/II Trial Schema Phase II Phase I Sorafenib Sorafenib + Bevacizumab R N = 88 Sorafenib + Bevacizumab KEY FINDINGS Patient Outcomes (N=17) BACKGROUND • HCC is considered a hypervascular tumor associated with VEGF overexpression • Sorafenib is an oral multi-kinase inhibitor with activity against the Ras/Raf/MEK/ERK signaling pathway as well as VEGF, platelet-derived growth factor (PDGF) receptor, Flt-3 and c-Kit • Sorafenib is the standard of care for unresectable HCC based on results of the SHARP trial • Bevacizumab is a monoclonal antibody that targets the vascular endothelial growth factor (VEGF) and blocks VEGF-induced angiogenesis • Preliminary from a phase II trial of single agent bevacizumab for patients with unresectable HCC showed promising activity • Combination bevacizumab and sorafenib may result in enhanced inhibition of VEGF-mediated angiogenesis *1 pt taken off study before the cycle one assessment SUMMARY AND CONCLUSIONS OBJECTIVES • Combination sorafenib (200 mg bid) and bevacizumab (2.5 mg/kg q.o.week) has an acceptable safety profile and is the recommended phase II dose • The phase II portion of this trial randomizing patients with unresectable HCC to sorafenib + bevacizumab versus sorafenib alone is ongoing • Translational components of this study examining the relationship between tumor biomarkers and circulating biomarkers of vascular response and clinical outcome treated with the sorafenib/bevacizumab combination are pending N = 17 Supported by NCI Grant ca25224 & Bayer Pharmaceuticals & Bayer’s REACH Program


















