Betty Smith
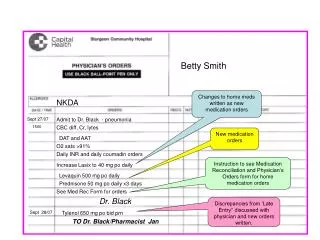
Betty Smith. Changes to home meds written as new medication orders. NKDA. Sept 27/07. Admit to Dr. Black - pneumonia. 1500. CBC diff, Cr, lytes. New medication orders. DAT and AAT. O2 sats >91%. Daily INR and daily coumadin orders.

Betty Smith
E N D
Presentation Transcript
Betty Smith Changes to home meds written as new medication orders NKDA Sept 27/07 Admit to Dr. Black - pneumonia 1500 CBC diff, Cr, lytes New medication orders DAT and AAT O2 sats >91% Daily INR and daily coumadin orders Instruction to see Medication Reconciliation and Physician’s Orders form for home medication orders Increase Lasix to 40 mg po daily Levaquin 500 mg po daily Prednisone 50 mg po daily x3 days See Med Rec Form for orders Dr. Black Discrepancies from ‘Late Entry’’ discussed with physician and new orders written. Sept 28/07 Tylenol 650 mg po bid prn TO Dr. Black/Pharmacist Jan
Nursing Instructions Physician Instructions Check ‘No home medications’ box if appropriate. Indicate time and date history obtained. Review and verify home medication history with patient. Update BPMH as needed to ensure accurate list. Betty Smith Indicate ALL sources of information used to obtain BPMH. Label and attach copies of information to prevent duplication of effort for next care provider. Indicate whether a home medication will be continued, discontinued or changed in the hospital by initialing the appropriate box. Sept 27, 2007 1030 x x Complete the BPMH Always talk to the patient and/or caregiver. Do not assume that any list is accurate. Note dates on any list supplied. Verify information with at least 2 sources if possible (more if required). x St Michael’s 472-4520 Document the reason for discontinuing or changing a home medication to improve communication to future care providers ASA 81mg po daily B Lipitor 20mg po daily B Sotalol 80mg po daily B Furosemide 20mg po daily B BP high-dose increase Warfarin 5mg po daily B Daily INR & orders Altace 5mg po daily B Draw a line from the last medication ordered to the physician signature box to prevent further medications from being ordered at a later time. Lactulose 15ml po qhs prn B Zopliclone 3.75mg po qhs prn B Sign immediately below your last entry. Nurse Efficient --------------------------------------------------- Late Entry Tylenol 650mg po bid prn A late entry to the BPMH can be made immediately below current information. Sign and date. Jan Pharmacists --------------------------Sept 28,07 Sign and date the physician's orders Dr. Black B Record self prescribed medications (cold remedies, herbals, vitamins) in this section. These will not be supplied in hospital unless specifically ordered by physician. Multivitamin 1 tab per day Sept 27, 2007 1500 hrs Write orders for changes in home medications and orders for NEW medications on the usual ‘Physician's Orders’ form. Note to ‘follow Med Rec orders’ Nystatin Suspension prescribed Sept 22-29 but discontinued by physician Sept 25 once problem resolved. Lactulose Rx 15 ml po bid but pt only takes 15 ml qhs prn. Tylenol for mobility 5-6 x/week Document important information for clarification of medications as needed.