Download
1 / 24
240 likes | 472 Vues
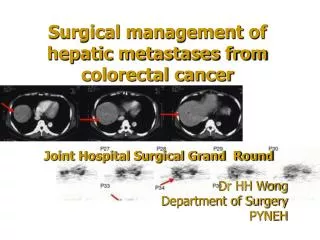
Neoadjuvant & Adjuvant Chemotherapy for Hepatic Colorectal Metastases : When to use it ?. SURGERY FIRST. May 30 , 2009. Hepatic resection is the only potentially curable treatment for colorectal liver metastases !!. General Agreement.

E N D
Neoadjuvant & Adjuvant Chemotherapy for Hepatic Colorectal Metastases : When to use it ? SURGERY FIRST May 30 , 2009
Hepatic resection is the only potentially curable treatment for colorectal liver metastases !! General Agreement
Neoadjuvant Therapy - Preoperative systemic therapy for resectable hepatic metastases. (Perioperative) Adjuvant Therapy – Systemic therapy post hepatic resection. **Conversion Therapy – Systemic therapy utilized for patients with unresectable hepatic metastases in an attempt to make the metastases resectable . DEFINITIONS: ASCO 2006 LIVER THINK TANK
An R0 resection. Minimally 2 adjacent liver segments spared. Vascular inflow & outflow, biliary drainage preserved. Remaining liver volume must be adequate. 20% normal; 30-60% chemo; 40-70% cirrhosis New Criteria of Resectability
“…limited data exists regarding the efficacy of adjuvant chemotherapy following resection for metastatic CR liver disease. Nevertheless, the panel recommends a course of active systemic chemotherapy … to increase the likelihood that residual microscopic disease will be eradicated.” NCCN GUIDELINES 2009
The Rationale for Systemic Treatment Post Hepatic Resection:Based on improved survival results in stage III colon cancer adjuvant trials!
ADJUVANT 5 Yr DFS : Chemo- 33.5% Surgery- 26.7% p=.028 Disease Free Survival ( %) Portier et al, Multicenter Randomized Trial of Adjuvant Fluorouracil & Folinic Acid Compared with Surgery Alone After Resection of Colorectal Liver Metastases: FFCD ACHBTH AURC 9002 Trial, J Clin Oncol 24; 4976-4981, 2006 Enrolled 173 Pts of planned 200 Pts over 10 yrs. Slow accrual /trial stopped.
Mitry,E et al, JCO, Vol. 26, No. 30, p.4910, 2008 No. PatientsRandomized Portier et al 173 Adjuvant FU/FA vs ( FCCD Trial)) Surgery alone (JCO 2006) Langer et al 129 SAME (ENG Trial) ( Proc ASCO 2002 )
Phase III Trial Resectable Hepatic Only Metastases • European Organization for Research & Treatment of Cancer (EORTC 40983) ASCO 2007; Lancet 371:1007,2008 Resectable Hepatic Metastases 1-4 ( 364 Pts) ↓ Randomize Pre ( 6 cycles) & Postop No Chemotherapy FOLFOX ( 6 cycles)
Progression-Free Survivalin Resected Patients HR= 0.73; CI:0.55-0.97, p=0.025 100 90 +9.2%At 3 years 80 LV5FU + Oxaliplatin Periop CT 70 60 50 42.4% 40 Surgery only 30 33.2% 20 10 0 (years) 0 1 2 3 4 5 6 O N Number of patients at risk : Treatment 104 152 85 59 39 24 10 Surgery 93 151 118 76 45 23 6 Pre&Postop CT
EORTC results based on sub population of patients randomized. A highly selected group of patients ( 1-4 metastases) Would patients with more metastases have the same results? Issue of post operative morbidity with chemotherapy before hepatic resection. MY MAIN DEFENSE!! ISSUES WITH PERIOPERATIVE TREATMENT ( EORTC)
Irinotecan – Steatohepatitis Oxaliplatin – Sinusoidal/vascular injury Acute & chronic clinical sequelae Biologics - ???? short & long term effects Bevacizumab – 6 to 8 wks before resection Liver regeneration (VEGF mediates hepatocyte & sinusoidal endothelial cell proliferation) Hemorrhage Morbidity is increased with prolonged course(>6 cycles) of chemotherapy (Nakano et al, Annals Surgery) (ASCO GI ,Abst# 295, 2009. > 9 cycles) Specific Chemotherapy Associated Hepatic Toxicity
Vascular Changes in Liver Post Systemic Chemotherapy Aloia et al, J Clin Oncol 24: 4983,2006 Vasodilation & Congestion Peliosis Cystic blood filled spaces in hepatic lobules Hemorrhagic Centrilobular Necrosis Nodular Regenerative Hyperplasia
Sinusoidal Injury /Dilatation Grade 0 – absent Grade 1 – centrilobular Involvement <1/3 lobular surface Grade 2 – centrilobular 1/3 - 2/3 Grade 3 – complete lobular involvement Grading according to: L. Rubbia-Brandt et al. Ann Oncol. 2004.
Sinusoidal Injury (SI) Secondary To Preoperative Chemotherapy Increases Post Hepatectomy MorbidityNakano et al, Annals Surgery ,2008 • 90 Pts –hepatectomy after preop chemotherapy. (Oxaliplatin - 62 Pts) • Incidence of SI was significantly higher in the Oxal. group ( 52%) vs other chemo (21%). • The morbidity of Gr. 3 & 4 was higher in pts. with SI ( 29%) than no SI (17%). (ns) • Post op complications: • transitory liver failure ,biliary fistula, cholangitis, intra abdominal collections ► increased LOS
Annals of Surgical Oncology 16:1247,2009 92 Pts. : 60 Pts. Chemo* before hepatic resection. 32 Pts. - No chemotherapy Analysis On Per Lesion Basis False+False -PPV Chemo Group 6.4%** 28.4% 93.5% No Chemo 0% 23.6% 100% Conclusion: Chemo reduces accuracy of CT for preop evaluation of CR LM. *Oxal – 30 Pts; Irinotecan - 15 Pts.
ACOSOG, NSABP, NCCTG, ECOG Phase III Trial Evaluating Perioperative vs Adjuvant Chemotherapy in Patients with Potentially Resectable Hepatic Colorectal Metastases
Schema Pt Population: RESECTABLE FOLFOX or FOLFIRI + Bevacizumab FOLFOX or FOLFIRI + Bevacizumab Liver Resection R 6 cycles 6 cycles FOLFOX or FOLFIRI + Bevacizumab Liver Resection 12 cycles
1)The results of perioperative chemotherapy with FOLFOX4 in addition to surgical resection are encouraging( 1-4 mets , good risk pts. ) but there is a better option► Hepatic resection first then chemotherapy!!! 2) Chemotherapy induced liver injury is real; patient selection, drug type & duration of chemotherapy must be taken into consideration. RESECTABLE COLORECTAL HEPATIC METASTASES Conclusions
CONCLUSIONS • 4) Surgeon / medical oncologist / pathologist must follow the patient as a multidisciplinary team. 5) Perioperative vs adjuvant - It is not just a matter of chemotherapy timing; It’s a matter of maintaining healthy liver parenchyma prior to surgery to minimize post op complications and maximize QOL.
Meaningful Progress in Cancer Care Results From Prospective Randomized Trials But Let’s Make Sure We Don’t Hurt Patients ! THANK YOU