Download
1 / 24

E N D
1. Double Hit B Cell Lymphoma Tzu-Fei Wang
3/30/2012
2. I have no disclosures
3. Non Hodgkin lymphoma subtypes
4. Aggressive B cell lymphoma Burkitt lymphoma
Diffuse large B cell lymphoma
the most common non-Hodgkin�s lymphoma
Prognostic factors
IPI (international Prognostic Index)
Age >60
ECOG PS = 2
Stage III or IV
Extranodal site >1
LDH > normal
Immunophenotype
Germinal-center B cells (GCB), activated B cells (ABC)
Gene rearrangement and protein expressions
BCL2, BCL6, c-MYC IPI initially published in 1993, revised in 2007IPI initially published in 1993, revised in 2007
5. The R-CHOP era- revised IPI
6. Double hit lymphoma An emerging concept as a subgroup of particularly aggressive B cell lymphoma
Rare, 3-5% of high grade B cell lymphoma
Most commonly c-MYC and BCL2 translocation
Often classified as �intermediate� or �gray zone� lymphoma in the new 2008 WHO criteria by morphology and immunophenotype.
Complex cytogenetics
very poor prognosis
Only case studies and series exist in the literature (>200 cases published)
A variety of therapies have been used, none proven to be superior than others. Double hit lymphoma can be found in a variety of morphologically diagnosed lymphoma, such as ALL, DLBCL, FL, IL, BL
~at least 60% are cmyc and bcl2 in the large Mitelman database of chromosome abberations in cancer
Can have other translocations too, such as bcl-6 and c myc, ccnd1 and cmyc. Double hit lymphoma can be found in a variety of morphologically diagnosed lymphoma, such as ALL, DLBCL, FL, IL, BL
~at least 60% are cmyc and bcl2 in the large Mitelman database of chromosome abberations in cancer
Can have other translocations too, such as bcl-6 and c myc, ccnd1 and cmyc.
7. World Health Organization Classification 4th Edition (2008) DLBCL, NOS
Common morphologic variants
Centroblastic, immunoblastic, anaplastic
Rare morphologic variants
Molecular Subgroups
Germinal centre B�Cell�Like (GCB)
Activated B�Cell�Like (ABC)
Immunohistochemical Subgroups
CD5�positive DLBCL
GCB
Non�GCB
DLBCL Subtypes
T-cell/histiocyte-rich large B-cell lymphoma
Primary DLBCL of the CNS
Primary cutaneous DLBCL, leg type
EBV positive DLBCL of the elderly
Many of these are included within trials of DLBCL
Prognostic findings may be influenced by the breakdown of pts within the cohort examined
Although we attempt to prognosticate across the entire entity of DLBCL, given the biologic differences between these different subtypes, perhaps we will never get it right until we create prognostic models for each subgroupMany of these are included within trials of DLBCL
Prognostic findings may be influenced by the breakdown of pts within the cohort examined
Although we attempt to prognosticate across the entire entity of DLBCL, given the biologic differences between these different subtypes, perhaps we will never get it right until we create prognostic models for each subgroup
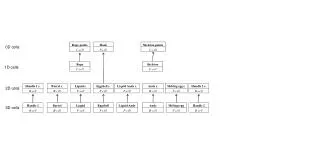
8. Distribution of morphologies according to breakpoints. For readability of the figure BCL3+/MYC+ and 9p13+/MYC+ DHs (n = 10) are omitted. SH indicates single hit.
The database contains all published cytogenetic data on a wide ariety of malifnanciesDistribution of morphologies according to breakpoints. For readability of the figure BCL3+/MYC+ and 9p13+/MYC+ DHs (n = 10) are omitted. SH indicates single hit.
The database contains all published cytogenetic data on a wide ariety of malifnancies
9. c-MYC and BCL2 BCL2 gene
Located on chromosome18q21
An apoptosis inhibitor
Most common- t(14;18)(q32;q21). t(2;18) or t(18;22)
t(14;18) is observed in 70-95% of FL and 20-30% of DLBCL
c-MYC gene
Located on chromosome 8q24
An accelerator of cell proliferation
Commonly- t(8;14)(q24;q32). t(2;8) or t(8;22)
8q24/MYC translocation is detected in 90-95% of BL, 41-80% of BLL, and up to 10% of DLCBL.
Next to ig heavy chain gene enhancer, resulting in bcl2 protein overexpressionNext to ig heavy chain gene enhancer, resulting in bcl2 protein overexpression
10. Morphology of double hit lymphoma
11. Double hit, morphology b cell, unclssifiable, features intermediate
Omental mass, starry sky
BM
Strongly pos for bcl2
Ki67>90%Double hit, morphology b cell, unclssifiable, features intermediate
Omental mass, starry sky
BM
Strongly pos for bcl2
Ki67>90%
12. Clinical features of double hit lymphomas
13. Clinical features of double hit lymphomas
14. Treatment and survival of DH lymphomas Rchop- 16.8, hd-3, chop like- 5, p=0.07
p=-pallative, ceep- cyclo, etoposide, epidoxorubicin, cisplain
COPADM- cyclo, vincristine, prednisone, doxorubicin, high dose MTX
IAM- ifos, etoposide, cytarabine, and mtX
Cyclobeap- cyclo, vincrisitne, bleomycin, etoposide, doxorubicin, prednisone
Ice- ifos, carbo, etoposide
Ivac- ifos, etoposide, high dose cytarabineRchop- 16.8, hd-3, chop like- 5, p=0.07
p=-pallative, ceep- cyclo, etoposide, epidoxorubicin, cisplain
COPADM- cyclo, vincristine, prednisone, doxorubicin, high dose MTX
IAM- ifos, etoposide, cytarabine, and mtX
Cyclobeap- cyclo, vincrisitne, bleomycin, etoposide, doxorubicin, prednisone
Ice- ifos, carbo, etoposide
Ivac- ifos, etoposide, high dose cytarabine
15. Overall survival by clonal karyotype: c-myc (�?�?�?�); other (�?�?�?�?�); and dual translocation (��).
British columbia cancer agency jan 1989-1996, n=39 (Snc-NB), 13 dual, 11 c myc, 15 others (1.8% of 2146 NHL)
Double hit no one survives beyond 7 months
Double hit group has more stage IV and more high IPI
Conclusion by the authors: double hit lymphoma may represent the most clinically aggressive lymphoma thus far, 13 years later, it is still trueOverall survival by clonal karyotype: c-myc (�?�?�?�); other (�?�?�?�?�); and dual translocation (��).
British columbia cancer agency jan 1989-1996, n=39 (Snc-NB), 13 dual, 11 c myc, 15 others (1.8% of 2146 NHL)
Double hit no one survives beyond 7 months
Double hit group has more stage IV and more high IPI
Conclusion by the authors: double hit lymphoma may represent the most clinically aggressive lymphoma thus far, 13 years later, it is still true
16. 19/394 (4.8%) abnormal karyotype with double hit
Advanced stage, high serum lactate dehydrogenase level, extranodal sites, B symptoms and bone marrow involvement were significantly more prevalent among patients with the dual translocation than among those in the other three groups. The CR rate was 53% (10/19) among patients with the dual translocation and 86.7% (325/375) among patients with other translocations (P=0.001).19/394 (4.8%) abnormal karyotype with double hit
Advanced stage, high serum lactate dehydrogenase level, extranodal sites, B symptoms and bone marrow involvement were significantly more prevalent among patients with the dual translocation than among those in the other three groups. The CR rate was 53% (10/19) among patients with the dual translocation and 86.7% (325/375) among patients with other translocations (P=0.001).
17. 54/1260 NHL (4%) selected lymphomas with cytogenetics and fish testing
Survival curves of patients with BCL2+/MYC+ lymphomas according to the timing of MYC+ rearrangement and treatment regimen. (A) Timing of MYC+ rearrangement: at diagnosis or at relapse. x-axis represents cumulative survival; y-axis, time (years). (B) Treatment regimen. ? represent long-term survivors; x-axis, cumulative survival; y-axis, time (years); Dx, diagnosis; R, rituximab; HD, high-dose chemotherapy with or without stem cell transplantation; and P, palliative.54/1260 NHL (4%) selected lymphomas with cytogenetics and fish testing
Survival curves of patients with BCL2+/MYC+ lymphomas according to the timing of MYC+ rearrangement and treatment regimen. (A) Timing of MYC+ rearrangement: at diagnosis or at relapse. x-axis represents cumulative survival; y-axis, time (years). (B) Treatment regimen. ? represent long-term survivors; x-axis, cumulative survival; y-axis, time (years); Dx, diagnosis; R, rituximab; HD, high-dose chemotherapy with or without stem cell transplantation; and P, palliative.
18. Low IPI also asso with better outcome (not shown0
Survival curves of patients with BCL2+/MYC+ lymphomas according to morphology, bone marrow involvement, MYC translocation partner, and BCL2 protein expression. Median overall survivals are shown in parentheses. (A) Morphology. (B) Bone marrow involvement. (C) MYC translocation partner. (D) BCL2 protein expression (clone 124). In all graphs, x-axis represents cumulative survival; and y-axis, time (years). BCLU indicates B-cell lymphoma unclassifiable; DLBCL, diffuse large B-cell lymphoma; BMneg, no bone marrow involvement with MYC+ lymphoma; BMpos, bone marrow involvement with MYC+ lymphoma; BCL2neg, no BCL2 protein expression by clone 124; BCL2pos, BCL2 protein expression by clone 124; and IG/MYC, MYC translocation involving one of the immunoglobulin genes.Low IPI also asso with better outcome (not shown0
Survival curves of patients with BCL2+/MYC+ lymphomas according to morphology, bone marrow involvement, MYC translocation partner, and BCL2 protein expression. Median overall survivals are shown in parentheses. (A) Morphology. (B) Bone marrow involvement. (C) MYC translocation partner. (D) BCL2 protein expression (clone 124). In all graphs, x-axis represents cumulative survival; and y-axis, time (years). BCLU indicates B-cell lymphoma unclassifiable; DLBCL, diffuse large B-cell lymphoma; BMneg, no bone marrow involvement with MYC+ lymphoma; BMpos, bone marrow involvement with MYC+ lymphoma; BCL2neg, no BCL2 protein expression by clone 124; BCL2pos, BCL2 protein expression by clone 124; and IG/MYC, MYC translocation involving one of the immunoglobulin genes.
22. Mechanism of poor outcomes Activation of MYC is directly responsible
but Burkitt lymphoma patients have much better prognosis
Synergistic action of MYC and BCL2
The effects of complex cytogenetics and additional genetic alterations
Le Gouill et al identified 22 DLBCL with complex cytogenetics but no dual translocation, better outcomes 6 die, 16 still alive with median f/u 17.5 mo (9-94), c/t median survival of 5 mo in double hit lymphoma in the same series6 die, 16 still alive with median f/u 17.5 mo (9-94), c/t median survival of 5 mo in double hit lymphoma in the same series
23. Conclusion Double hit lymphomas are heterogeneous in morphology, clinical presentation, and outcomes.
They are generally associated with very poor prognosis.
No regimen is proven to be superior than others in this disease, although the tendency is to intensify therapies.
Innovative therapies are needed.
Comprehensive analysis of the status of Bcl2 and c-myc should be incorporated into the diagnosis of aggressive B cell lymphoma. We don�t do transplant right off the back.
R-epoch or hyperCVAD as first line?We don�t do transplant right off the back.
R-epoch or hyperCVAD as first line?
24. References Aukema SM, Siebert R, Schuuring E, et al. Double-hit lymphoma. Blood 2011;117(8):2319-2331.
Bertrand P, Bastard C, Maingonnat C, et al. Mapping of MyC breakpoints in 8q24 rearrangements involving non-immunoglobulin partners in B-cell lymphomas. Leukemia 2007:21:515-523.
Johnson NA, Savage KJ, Ludkovski O, et al. Lymphomas with concurrent BCL2 and MYC translocations: the critical factors associated with survival. Blood 2009;114(11):2273-2279.
Kanungo A, Medeiros LJ, Abruzzo LV, Lin P. Lymphoid neoplasms associated with concurrent t(14;18) and 8q24/c-MYC translocation generally have a poor prognosis. Mod Pathol 2006;19(1):25-33.
Le Gouill S, Talmant P, Touzeau C, et al.The clinical presentation and prognosis of diffuse large B-cell lymphoma with t(14;18) and 8q24/c-MYC rearrangement. Haematologica 2007;92(10):1335-1342.
Li S, Lin P, Dayad LE et al. B-cell lymphomas with MUC/8q24 rearrangements and IGH2BCL2/t(14;18)(q32;q21): an aggressie disease with heterogeneous histology, germinal center B-cell immunophenotype and poor outocme. Modern Pathology 2012;23:145-156.
Macpherson N, Lesack D, Klasa R, et al. Small noncleaved, non-Burkitt�s (Burkitt-like) lymphoma: cytogenetics predict outcome and reflect clinical presentation. J Clin Oncol 1999;17:1558-1567Mitelman F, Johansson B, Mertens F, editors. Mitelman Database of Chromosome Aberrations and Gene Fusions in Cancer (February 2010). [Accessed September 2, 2010]. http://cgap.nci.nih.gov/Chromosomes/Mitelman.
Niitsu N, Okamoto M, Miura I, Hirano M. Clinical features and prognosis of de novo diffuse large B-cell lymphoma with t(14;18) and 8q24/c-MYC translocations. Leukemia 2009;23(4):777-783.
Sehn LH, Berry B, Chhanabhai M, et al. The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP, Blood 2007;109:1857-1861.
Shipp MA, Harrington DP, Anderson JR, et al. A predictive model for aggressive Non-Hodgkin�s lymphoma. N Engl J Med. 1993;329:987-994.
Snuderl M, Kolman OK, Chen YB, et al. B-cell lymphomas with concurrent IGH-BCL2 and MYC rearrangements are aggressive neoplasms with clinical and pathologic features distinct from Burkitt lymphoma and diffuse large B-cell lymphoma. Am J Surg Pathol 2010;34(3):327-340.
Tomita N, Tokunaka M, Nakamura N, et al. Clinicopathological features of lymphoma/leukemia patients carrying both BCL2 and MYC translocations. Haematologica 2009;94(7):935-943.