Download
1 / 19
200 likes | 769 Vues
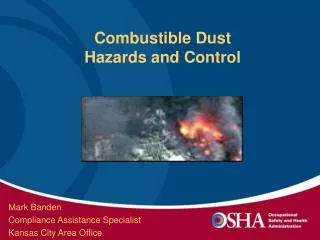
1. Organic dusts Examples: Cotton, flax and soft hemp dusts Byssinosis Sugar cane dusts Bagassosis Hay moulds Farmer’s lung Feathers, wool, furs : Occupational asthma Wheat grains, gum : Acacia, red cedar : Wood, piperazine :. Byssinossis.

E N D
1. Organic dusts • Examples: Cotton, flax and soft hemp dusts Byssinosis • Sugar cane dusts Bagassosis • Hay moulds Farmer’s lung • Feathers, wool, furs : • Occupational asthma • Wheat grains, gum : • Acacia, red cedar : • Wood, piperazine :
Byssinossis • characterized by tightness or heaviness in the chest on the first day back at work after holiday in cotton workers after many years of exposure in the average 3-10 years. This tightness or heaviness occurs some hours after starting work on the first day back at work after holiday and later on the other days of the week. The susceptible worker notices a tightness of his chest and shortness of breath one to six hours after beginning of work on Saturday. This is one point differentiating the condition from bronchial asthma as the asthmatic usually develops his attack immediately he comes in contact with the allergen. Tightness commonly increases in degree until worker leaves the mill. • In the final stage of the disease, the continued strain on the right side of the heart lead ultimately to heart failure.
Investigation • 1. Lung functions • Forced expiratory volume in the first second (F.E.V.I.O) remains the most informative and practical test for the assessment of exposed workers. After about 6 hours of exposure to cotton dust a significant fall in F.E.V 1.0 occurs in most individuals who have permanent as well as those with transient respiratory disability (all grades) • 2) X – rayLung: • No change • 3) Intradermal test: • Not helpful
Farmer’s Lung • It occurs due to swallowing of moldy hay that contains the infected source of antigen (Micropolyspora Faeni and Thermoactinomyces vulgaris). The disease takes two forms; acute and chronic. Acute disease follows in a few hours after exposure to mouldy hay or grain dust. It is potentially reversible with complete recovery. Chronic disease may occur after repeated episodes of acute diseases that ultimately fail to resolve or it may develop insidiously after repeated exposure to small amount of antigen over a long period. It is not reversible and usually progressive.
Bagassosis • Bagasse is the fibrous cellulose residue of sugar cane stalk after it has been crushed and the juice extracted. The symptoms, physical signs and radiological appearance of both acute and chronic disease are similar to those of farmer’s Lung. As in the case of farmer’s lung the majority of cases with acute disease recover spontaneously in 4-12 weeks after being removed from exposure. Corticosteroids in adequate doses hasten clinical recovery.
Bird Breeder’s (Fancier’s Lung • This extrinsic allergic alveolitis which is caused by avian protein antigens is similar to farmer’s lung in having acute and chronic forms with the same clinical, physiological, radiological and pathological features. It is recognized to be related to exposure to the dust of the droppings of pigeons, parrots and hens. It has been reported in children as well as in adults.
1)Mineral Dusts • These types of dusts are further classified according to their effect on the body into: • A: Inert dusts • B: Fibrogenic dusts causes lung fibrosis.
Examples of pneumoconiosis • Iron: Siderosis • Tin: Stannosis • Barium:Baritosis • Coal:Antheracosis: • Silica: silicoses • Asbestos: asbstoses
Silicosis • Definition: Silicosis is a disease resulting due to breathing air containing silica characterized anatomically by generalized fibrotic changes and the development of military nodulation in both lungs, and clinically by shortness of breath, decreased chest expansion, lessened capacity for work, absence of fever, increased susceptibility to tuberculosis (some or all of these symptoms may be present) and by characteristic X-ray findings.
Sources of exposure to silica Exposure is encountered in metal mining, quarries tunnel construction, building, shaping and blasting, granite crushing, drilling, pottery and clay manufacturing. Glass and ceramic industries, foundries, manufacture of brick, road construction, and reclamation of land in the desert …etc.
Factors important in the development of silicosis • 1.- Concentration of dust in the breathing air. • 2.- Concentration of silica in the dust. • 3.- Duration of exposure by using the formulae particle years or M.P.P.C.F./year. (million particle per cubic feet/year). • 4.- Particle size • Larger than 10 microns retained in the nose and fall to the ground readily. • 5-10 microns retained in the upper respiratory tract and expelled by cough. • 3-5 microns retained in bronchi and large non-respiratory bronchioles and expelled by cough. • Less than 3 microns pass to respiratory alveoli and causes fibrosis. It is the dangerous particle size. • 5.- Presence of pre-existing disease e.g.: TB • 6.- Individual susceptibility.
Signs and Symptoms • The earliest cardinal symptom is dyspnea on severe exertion. This becomes more and more apparent on slight effort as the disease advances. Cough is short, irritating unproductive and more troublesome at bedtime or in the morning. When sputum occurs it is usually tough, viscid and little in quantity. There is usually no haemoptysis unless tuberculosis is present.
Diagnosis • 1.- History of occupational exposure to silica dust. • 2.- Clinical examination of the workers. • 3.- Pulmonaryfunction tests • They are important for the detection of early changes. Decrease in vital capacity, maximum breathing capacity and exercise oxygen uptake. • 4.- Chest X-Ray Film • The most important tool for diagnosis of silicosis should be differentiated from more than 100 different disorders cause military shadows in chest X-ray
Sources of exposure to asbestos • Textile industry to manufacture cloth rope, theatre curtains. • Paper, cardboard, covering agents, cements • Brakes for the cars. • Electric insulators. • Insulate pipes transmitting superheated steam. • Cover electric wiring, to make insulating gloves, firemen’s clothes. • Mining, sorting, extracting, carding, spinning and weaving of asbestos
Signs and Symptoms • Breathlessness on effort is the most important first symptom, slight at first and then increasing in severity. Cough is a late symptom usually dry sometimes distressing. Clubbing of fingers and toes may occur in 75% of cases. Warts and corns may be present on the skin of the dorsal and palmar surfaces of the hands and forearms of asbestos workers. Fine intra pulmonary adventitious sounds and crepitations may be heard on the base of the lungs. • In advanced cases or when carcinoma supervenes; lassitude, haemoptysis, chest pain and loss of weight are important signs and symptoms.
Diagnosis: History of exposure • Type, length, size of fibres and duration of exposure are all important factors. Amosite may not be as fibrogenic as chrysotile. Fibres of one or less microns in width and up to 10-15 U in length were the most pathogenic. Minimal exposures among wives dusting their husbands miners cloths were reported to lead to asbestosis and even lung cancer. However, generally speaking exposure time is usually many years before the production of manifested clinical changes. • 2.Peculiar clinical signs and Symptoms • Specially clubbing of fingers, skin corns, lung crepitations …etc
Investigations • a) Sputum: asbestos bodies • b) E.S. Rate: raised especially in advanced cases. • c) Serology: in 25% of cases presence of positive rheumatoid factor. • d) Lung function • Vital capacity: the most sensitive test in early detection of asbestosis as well in follow up of progression of the disease. It may be impaired some 10 to 15 years before moderate or advanced fibrosis is apparent radiographically. • Diminish gas transfer. • Diminish compliance. • e) X-ray chest: • It shows one or more of the three manifestations • Pulmonary interstitial fibrosis. • Pleural fibrosis and plaques. • Pleural effusion.
Prevention and control Substitution is the only wholly satisfactory solution to the problem. Asbestos is now mostly replaced by glass wool and other harmless substances. Other control measures will be listed as discussed before. Regression of fibrosis was not observed after the beginning of fibrosis. It is therefore, agreed that medical controls are only palliative and emphasis should be given to control of dust.