
Abstract
Base Rates of Effort Test Failure in Veterans Diagnosed with Dementia: Alternative Cutoffs to Reduce False Positives in a Clinical Sample John Denning, Ph.D . and Randy Petersen, Ph.D. Tennessee Valley Healthcare System, Alvin C. York VA Medical Center, Murfreesboro , Tennessee. Abstract

Abstract
E N D
Presentation Transcript
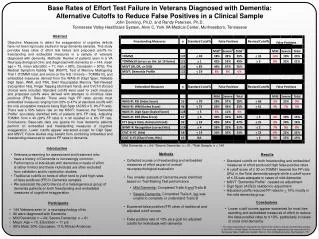
Base Rates of Effort Test Failure in Veterans Diagnosed with Dementia: Alternative Cutoffs to Reduce False Positives in a Clinical Sample John Denning, Ph.D. and Randy Petersen, Ph.D. Tennessee Valley Healthcare System, Alvin C. York VA Medical Center, Murfreesboro, Tennessee Abstract Objective: Measures to detect the exaggeration of cognitive deficits have not been rigorously studied in large dementia samples. This study provides base rates of effort test failure and proposed cutoffs for freestanding and embedded measures in a sample of veterans diagnosed with dementia. Methods: Review of patients seen in a VA Neuropsychological clinic and diagnosed with dementia (n = 144, mean age = 73, mean education = 11; men = 98%, Caucasian = 90%). The Medical Symptom Validity Test (MSVT), Test of Memory Malingering Trial 1 (TOMM1 total, and errors on the first 10 items – TOMMe10), and embedded measures derived from the WAIS-III (Digit Span, Reliable Digit Span, WMI, and PSI), Brief Visuospatial Memory Test-Revised (recognition hits), Finger Tapping (dominant hand), and CVLT-II (forced choice) were included. Standard cutoffs were used for each measure and proposed cutoffs were derived with attempts to minimize false positives (FPs). Results: There were high FP rates across most embedded measures ranging from 28% to 47% at standard cutoffs with the only acceptable measure being Digit Span (ACSS ≤ 5, 8% FP rate). There was a 56% failure rate on the MSVT; however, the “Dementia Profile” accurately identified 94% of patients (6% FP rate). Adjusting TOMM1 from ≤ 40 (29% FP rate) to ≤ 30 resulted in a 9% FP rate. Conclusions: Base-rate data are sparse for how dementia patients perform on embedded and freestanding measures of cognitive exaggeration. Lower cutoffs appear warranted except for Digit Span and MSVT. Future studies may benefit from combining embedded and freestanding measures to reduce FP rates in dementia. 1Mild Dementia: n = 64; 2Severe Dementia: n = 61; 3Total Sample: n = 144 • Introduction • Veterans presenting for assessment and treatment who have a history of Dementia is increasingly common. • Performance of individuals with dementia on tests of effort is rather limited and these individuals are often excluded from validation and/or replication studies. • Traditional cutoffs on tests of effort tend to yield high rates of false positives (FP) in Dementia samples. • We assessed the performance of a heterogeneous group of dementia patients on both freestanding and embedded measures of cognitive exaggeration • Methods • Collected scores on freestanding and embedded measures of effort as part of overall neuropsychological evaluation • Two smaller subsets of Dementia were identified based on Trail Making Test performance • Mild Dementia: Completed Trails A and Trails B • Severe Dementia: Completed Trails A, but was unable to complete or understand Trails B • Examined false positive (FP) rates of traditional and adjusted cutoff scores • False positive rate of 10% as a goal for adjusted cutoffs for individuals with dementia • Results • Standard cutoffs on both freestanding and embedded measures of effort produced high false positive rates • A cutoff score of ≤ 30 on TOMM1 lowered the FP rate (9%) in the Total dementia sample while a cutoff score of ≤ 35 was adequate in cases of mild dementia • MSVT “Dementia Profile” needed no adjustment • Digit Span (ACSS) needed no adjustment • Adjusted cutoffs reduced FP rates to < 10% mostly in the mild dementia group • Conclusions • Lower cutoff scores appear warranted for most free standing and embedded measures of effort to reduce the false positive rates to ≤ 10%, particularly in cases of more mild dementia • Participants • 144 Veterans seen in a neuropsychology clinic • All were diagnosed with Dementia • Mild Dementia: n = 64; Severe Dementia: n = 61 • Mean: Age = 73, Education = 11 yrs • 98% Male, 90% Caucasian, 11% African American * The views expressed in this poster are those of the authors and do not reflect the position of the DVA or United States Government. This work was supported by the resources at the Tennessee Valley Healthcare System, Alvin C. York VA Medical Center, Murfreesboro, TN


















