Download
1 / 47
470 likes | 567 Vues
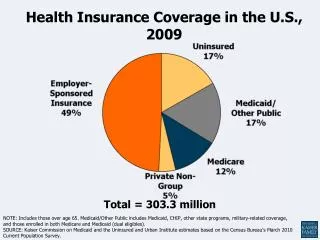
Employer Provided Health Insurance in the U.S. November 2 - 9, 2005. What is Group” Insurance?. A technique under which many individuals (and possibly their dependents) are insured under a single policy issued to another entity “Individuals” are usually employees

E N D
Employer Provided Health Insurance in the U.S. November 2 - 9, 2005
What is Group” Insurance? • A technique under which many individuals (and possibly their dependents) are insured under a single policy issued to another entity • “Individuals” are usually employees • “Another entity” is usually the employer • Predominant method of providing health insurance, life insurance disability, insurance, and dental insurance
Group Insurance Characteristics • Group Contract • Provides coverage to many people under one contract. Individuals receive a certificate of insurance. • Experience Rating • Actual claims experience of the group may be used to determine future premiums • Group Underwriting • Underwriting is evaluation of applicant to determine price • Members of a group not required to show evidence of insurability
Group Insurance & Adverse Selection • Adverse selection can be quite costly and can even lead to “unraveling” of the insurance market • By providing insurance to an entire group, it automatically pools higher and lower risk people together • Note: can still have selection by “group” • Coal miners versus stock analysts • Role of experience rating
“Desirable” Groups to Insure • Exist for reason other than obtaining insurance • Reasonable and steady turnover • Persistent – will be around for a while • Minimize individual participation choice • Favorable eligibility provisions • Good prior experience
Other Underwriting Factors • Size of the group • Composition of group (age, sex, income) • Industry • Geography
Eligible Groups (in most states) • Often a minimum number of persons to be considered a group • Common in life insurance policies (often 10 people) • About ½ of states have min. for health (5 - 10 people) • Most states approve the following groups: • Individual employer groups • Negotiated Trusteeships • Trade associations • Labor union groups • Some also allow “Multiple employer welfare arrangements” (MEWA)
State Regulation • McCarran-Ferguson Act (1945): gives the states substantial regulatory authority in the area of insurance • Nearly all regulation done at the state level • National Association of Insurance Commissioners (NAIC) tries to encourage uniformity of regulation, but much variation exists
Regulation • States regulate contract provisions • States may impose limitations on benefits • Taxes on insurer of approx 2% of premiums often levied within a state. Note: HMOs not subject to this tax • Jurisdiction – doctrine of comity
Benefit Mandates (examples) • California • In vitro fertilization, diabetic education, accupuncture • Connecticut • Dentists, dependent students, naturopaths • Wisconsin • Alcoholism treatment, chiropractors
Federal Legislation • Age Discrimination in Employment Act • Pregnancy Discrimination Act • ERISA • Americans with Disabilities Act • Health Maintenance Organization Act • COBRA • Health Insurance Portability and Accountability Act • Mental Health Parity Act • Family and Medical Leave Act • Many others …
Brief History of HI in US • Health insurance largely non-existent before Great Depression • Blue Cross – run by hospitals, guaranteed a certain number of hospital days per year in return for annual premium • Blue shield – for physician payments • Private insurance took off during/after WWII • During price controls, firms were allowed to offer health benefits to compete for workers • Blue cross had been profitable • Tax benefits
Brief History, continued • Medicare (elderly) and Medicaid (poor) introduced in 1960s • Group health insurance receives very favorable tax treatment • Deductible at corporate level (no corp tax) • Not taxed at individual level by federal or state income tax, or Social Security tax • A major reason for the predominance of an employer based health insurance system • 2005 Presidential tax reform panel recommends limiting the tax benefits
Why Do We Care About Insurance? • Many medical expenditures are highly uncertain & (partially) unpredictable imposes significant financial risk on individuals • Basic economics / insurance theory suggests that risk averse individuals are made better off (have higher utility) when they can insure against risk
Concentration of Health Spending in U.S. Population, 2002 Source: www.kff.org
Concentration of Health Spending in U.S. Families, 2002 Source: www.kff.org
Insurance Theory in Brief • Liquidity constraints: it is difficult to borrow when sick (may not live to repay!) • It is not optimal to save for low probability, high cost outcomes (may never occur) • Insurance allows you to reduce consumption only by the annual premium (the average cost of care in population) rather than being exposed to uncertainty • If insurer covers lots of people with uncorrelated risks, then insurer can predict average costs reasonably well
The Fundamental Trade-off • Risk Spreading vs. Incentives: Health insurance involves trade-off between risk spreading and providing incentives to use health care efficiently • By efficiency, we mean use health care when the social gains exceed the social costs • Increasing the generosity of insurance spreads risk more broadly, but also may lead to increased average losses • “Moral hazard” • “Principal agent problems”
Moral Hazard • A form of “hidden action” that arises from insurance company’s inability to monitor and control behavior • Individuals are more likely to seek out treatment if they do not pay for it themselves • Optimal insurance contracts would only pay for care that the individual would have chosen had he/she not been insured • Very difficult to monitor!
Is MH Really a Problem? • The issue: Is demand for medical care sensitive to price? • Evidence: Most economists agree that there is a moderate price elasticity of demand • Reasonable estimate is –0.2 • A 10% increase in out of pocket costs decreases health expenditures by 2% • Ex: If insurance lowers out of pocket costs by 80%, then expenditures will rise 16%
Policy Features to Address MH • Deductibles: amount an individual must pay before insurance company pays anything • Coinsurance rates (co-payments): The percentage of the total bill above the deductible paid by the patient • Stop loss amounts: Coinsurance paid until stop loss is reached – maximum out of pocket payment in a year • Policies may also cap various types of expenditures (e.g., only 8 mental health visits per year)
Principal-Agent Relationships • Issues that arise when the principal expects the agent to act in principal’s best interest • Examples: PrincipalAgent Patient Doctors Shareholders Firm managers Defendant Defense attorney • Principal Agent problems arise when the interest of the principal and agent are in conflict
Patients, Doctors and Insurers • Traditional insurance – insurer pays a fixed amount based on procedure / treatment provided • Patient & doctor incentives are aligned • Doctor’s Hippocratic oath is to what is in best interest of patient • Insurers interest not well-served: Dr gets paid for procedure, patient pays nothing, so incentives exist to maximize health outcomes with no concern for cost
Changing Relationships • New forms of insurer/provider relations are changing the incentives • Doctors now have responsibilities to other providers, insurers, not just patients • Incentives to hold down expenditures may ultimately enhance aggregate patient well-being • But this can lead to conflicts about what constitutes appropriate care • When others are sick, you want resources targeted efficiently • When you are sick, do you want your doctor thinking about the bottom line?
Types of Policies • Indemnity – basically “fee-for-service” • Managed Care • Preferred Provider Organizations (PPOs) • Health Maintenance Organizations (HMOs) – fully integrate insurance and provision
Indemnity Insurance • Traditional insurance is known as indemnity insurance • Pays a fixed amount of money for a particular condition when the individual is sick • Amount paid is the “appropriate” amount for the person’s disease
Traditional Plan Overview • Prior to mid-1970s, most employees were covered by traditional or indemnity plans • Patients had freedom to choose provider • Few attempts at controlling costs • Today, even the traditional plans have many managed care features to control costs, influence behavior of patients and focus more on preventative care • Traditional plans now cover a minority of employees (14% by some estimates) but it varies widely by state
Typical Indemnity Plan • Basic medical coverage • Hospital expense benefits • Surgical expense benefits • Physician expense benefits • Vision care • Prescription drugs • Hospice care • Major medical (for catastrophic events)
Total payment $ paid Cost sharing under Indemnity insurance Insurer payment Patient payment Stop loss deductible Total $ expenditure
Regulations • Some states mandate coverage of mental illness, alcoholism, drug addiction, etc • Mental Health Parity Act (>50 employees) • Pregnancy Discrimination Act requires firms with >15 employees to treat pregnancy, childbirth, etc the same as other conditions • Since 1998, “Newborns’ and Mothers’ Health Protection Act” – must cover hospital stays for 48 hours following vaginal delivery, 96 hours for cesarean (for both mother and child)
Managing Care in Traditional Plans • “Managed care” simply means the insurer influences type and scope of care received • Pre-certification, 2nd opinions, etc. • Pre-approval of visits to specialists • Increased benefits for preventative care • So why are these traditional plans not called managed care plans? • Few restrictions on access to providers
Managed Care • Preferred Provider Organizations (PPOs) – forms network of Drs, hospitals, pharmacies • Out of network care much more expensive • Health Maintenance Organizations (HMOs) – fully integrate insurance and provision • Group/staff HMOs – physicians are salaried employees (e.g. Kaiser) • Independent Practice Associations (IPAs) or Network Model HMOs • Do not have own employees, but contract with providers • Stringent review procedures
Typical Group Health Provisions: Eligibility • Covered position • Probationary period • Full time • Actively at work • Eligibility and plan replacement • Covered by previous plan • Eligible classification • Special situation: preexisting condition • Treatment of deductible
Dependent Eligibility • Eligible dependents • spouse • children < specified age, disabled any age • Employee must usually be covered • Enrollment window if contributory • 31 days typical • new job • new insurance plan • dependents for first time • yearly open enrollment period • New dependents covered if others are
Coordination of Benefits • Plan with COB provision pays first • Coverage as employee pays before coverage as dependent • Children with two parents living together birthday rule: policy of parent with earliest birthday • Other rules for different family structures
Termination of Coverage • Termination of coverage of employee • employment terminates • employer cancels coverage • employee ceases to be eligible • maximum benefit is reached • employee quits making contributions • Termination of coverage of dependents • dependent ceases being a dependent • employee’s coverage ceases • dependent hits maximum benefit • employee quits making contributions
COBRA • Consolidated Omnibus Budget Reconciliation Act of 1985 • Requires that health plans allow employees and certain beneficiaries to elect to have their current HI coverage extended at group rates for up to 36 months following a “qualifying event” • Death of employee, termination, change in workers status to part time, divorce, employee eligibility for Medicare (spouse and kids), child ceases to be a dependent
COBRA: Coverage Ceases • Termination or part time: 18 months • Social Security disability: 29 months • Other qualifying events: 36 months • Immediately if: • don’t pay portion of premium • group plan terminates • covered by another plan
COBRA Misc. • Must be offered continuation • Not automatic coverage • Individual must pay premium, but limited to 102% of cost for active employee (150% for months 19-29 if Social Security disabled) • COBRA has proven costly to employers • Adverse selection: only elected by 20% of eligibles, and they have costs that are 150% - 200% of claim costs for active employees
Preexisting condition • Mental or physical condition for which medical advice, diagnosis, care or treatment was recommended or received within the 6-month period ending on enrollment date • Plans typically allowed to put restrictions in place for 12 months • HIPAA: Health Insurance Portability and Accountability Act of 1996 • Increase labor mobility / reduce “job lock” • Use evidence of prior insurance coverage to reduce / eliminate length of preexisting condition exclusion
Health Insurance Portability and Accountability Act (HIPAA) of 1996 • Pre-existing conditions: exceptions • no 12 month period for • pregnancy: if no lapse in coverage • newborns and adopted children • if covered within 30 days • Premiums: can not be higher for pre-existing conditions • Coverage proof: former employer • Effective date: June 30, 1997
Health Savings Account • HSAs are new, effective January 1, 2004 • Pay for current and future health expenses on tax free basis • Eligibility: • Must be covered by high deductible health plan • Must not be covered by other health insurance • Not eligible for Medicare • Not dependent on someone else’s return
HSA Definitions • $1000 < deductible < $2000 • Out of pocket < $5000 (indiv) or $10k (family) • Contributions made by employer, employee or both – contributions are aggregated • Max contribution is lesser of deductible or $2,600 (indiv) or $5,150 (family) • Can be used for medical expenses, or after 65, for Medicare premiums, etc.
HSA Debate • Idea is to provide incentives for individuals to control costs – money that is not used can be used to reduce future costs • Bundling with high-deductible plan provides catastrophic coverage • Should these be extended more broadly?
The Future of U.S. Health Care in a Global Market • G.M. article • Can GM remain globabally competitive with such high health care costs? • If not, what should GM do? • Whose responsibility is it? • WalMart articles • Is WalMart “anti-worker” for not providing generous health care packages? • What do you think about WM employees using means-tested programs like Medicaid?