Download
1 / 29
360 likes | 607 Vues
WOMEN AND HEART DISEASE . M. Carolina Karam Demori, MD. OUTLINE. Statistics Gender Disparities Acute Coronary Syndrome CABG Surgery & Outcomes Device Implantation & Outcomes Calcium Supplements & Risk of CVD Vitamin D & Risk of CVD Guidelines Update 2011. STATISTICS.

E N D
WOMEN AND HEART DISEASE M. Carolina Karam Demori, MD
OUTLINE • Statistics • Gender Disparities • Acute Coronary Syndrome • CABG Surgery & Outcomes • Device Implantation & Outcomes • Calcium Supplements & Risk of CVD • Vitamin D & Risk of CVD • Guidelines Update 2011
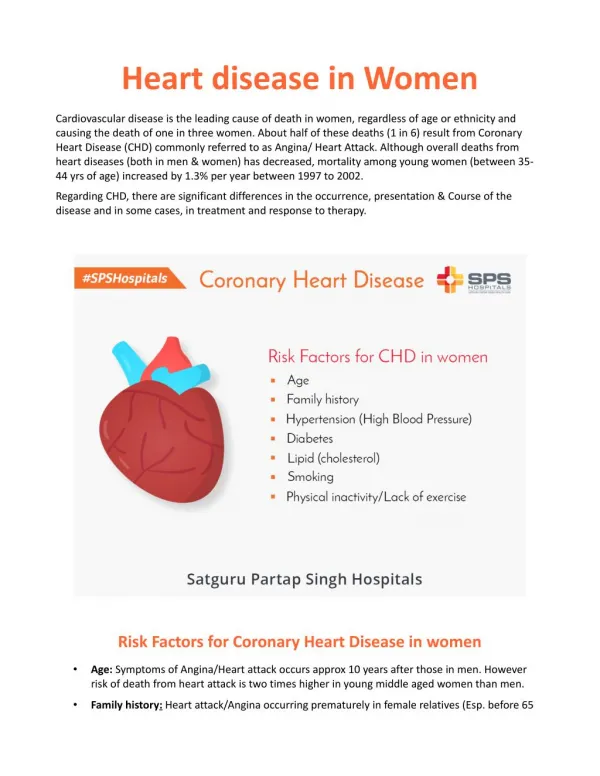
STATISTICS • Cardiovascular disease (CVD) is the most common cause of death in women • It accounts for a little over a 1/3 of all deaths • The lifetime risk of CVD in women is very high, more than 1 in 2 women at age 40 • More women than men die every year from CVD Heart Disease and Stroke Statistics 2011 Update: A Report from the AHA. Circulation 2011
STATISTICS CVD disease mortality trends for males and females(United States: 1979-2007). Source: NCHS and NHLBI.
STATISTICS • However, coronary heart disease (CHD) death rates in US women 35 to 54 y/o now appear to be increasing • Likely because of the obesity epidemic • Affecting nearly 2 of every 3 US women >20 y/o • 75.1% of Mexican American women Heart Disease and Stroke Statistics 2011 Update: A Report from the AHA. Circulation 2011
STATISTICS • Awareness of CVD as the leading cause of death among women is only 57% • Significantly improved from 1997 – only 30% • Even lower among Hispanic42%, African American 43%, and Asian women 34% Heart Disease and Stroke Statistics 2011 Update: A Report from the AHA. Circulation 2011
GENDER DISPARITIES Acute Coronary Syndrome • Women experience milder and atypical symptoms • Present later in the course of symptoms3 • Have more comorbidities3 • Frequently have high-risk clinical findings of HF and tachycardia3 • Have increased early death4,5 – only during STEMI6 according to latest report 3 McGuire et al. A companion to Braunwald’s Heart Disease 2003 4 Vaccarino et al. Circulation 1995 5 Hochman et al. N Engl J Med 1999
GENDER DISPARITIES • Women are less likely to receive: • Early medical treatments • Acute reperfusion therapies • Timely pharmacological and mechanical reperfusion therapies • Invasive procedures Aspirin & β- blockers 6 Jneid et al. Sex Differences in Medical Care and Early Death after Acute Myocardial Infarction. Circulation 2008:118:2803-2810
GENDER DISPARITIES • Women who present with CP or ACS are more likely than men to have: • Less severe obstructive coronary lesions7 • Vasospastic disease7,8 • Smaller vessels • In situ coronary thrombosis8 7 Braunwald, et al. ACC/AHA Guidelines Update for the management of patients with unstable angina and non-ST-elevation MI. 2002 8 Anderson et al. Circulation 2007;115
GENDER DISPARITIES CABG Surgery • Men were considerably more likely than women to get a CABG procedure9 • Women had a significant higher in-hospital mortality rate than men even after controlling for multiple factors9,10 Five-year National Data from 1998-2002 & The CCORP from 2003-2004 9 Becker ER, Rahimi A. J Natl Med Assoc2006;98(11): 1729-1739 10 Bukkapatnam RN, et al. Am J Cardiol 2010;105:339-342 11 Kim C, et al. Clin Cardiol 2007;30: 491-495
GENDER DISPARITIES • Reasons for increased in-hospital mortality: • Women have higher risk in terms of age, DM, HF, and renal disease10,11 • A greater proportion of women than men had urgent or emergent CABG which is associated with higher mortality10,11 • Women have smaller vessels – greater periprocedural complications11 • Lower use of internal mammary artery graft which has been associated with improved outcomes10,11 • Possible implication of coronary microvascular disease11
GENDER DISPARITIES Cardiac Device Implantation • A prospective multicenter registry (n = 26,264) aimed to investigate the impact of gender and race on rates of implantation of pacemakers and ICDs in patients with reduced LV function12: • Female gender was independently associated with decreased implantation of any device 12 El-Chami MF, Hanna IR, Bush H, Langberg JJ. Heart Rhythm. 2007 Nov;4(11):1420-6
GENDER DISPARITIES Cardiac Device Implantation • 161,470 patients undergoing firs-time ICD implantation13 • After accounting for demographic, clinical and procedural differences, women had 71% higher odds of experiencing a major adverse event (perforation, lead dislodgment, hemo and pneumothorax, coronary venous dissection) • Smaller body size is a possible explanation – smaller blood vessel diameter and thinner right ventricular wall Data from the National Cardiovascular Data Registry ICD Registry from 2006-2007 13 Peterson PN, et al. Circulation 2009;119:1078-1084
GENDER DISPARITIES Conclusions: • Women are significant less likely to get appropriate live-saving medical, surgical, and device therapies • Women have a higher complication rate during revascularization procedures and device implantation, including greater in-hospital mortality during CABG
CALCIUM & HEART DISEASE The Calcium Supplement Controversy15 • Observational studies suggest that high Ca++ intake might protect against vascular disease • Several interventional studies showed improvement in some vascular risk factors, such as increase in the HDL/LDL ratio • In contrast, Ca++ supplements accelerate vascular calcification and increase mortality in patients with renal failure 15 Bollard MJ, et al. BMJ 2010;341:c3691
CALCIUM & HEART DISEASE • A 5-year RCT of Ca++ supplements in healthy older women reported an increase of borderline significance (p=0.05) in the rate of MI in the Ca++ group • A recent meta-analysis included data from 11 RCT trials of Ca++ supplements (≥500 mg/day) without vitamin D, 88% women, mean age 69 y/o • Calcium supplements were associated with approximately 30% increase in the incidence of MI 15 Bollard MJ, et al. BMJ 2010;341:c3691
CALCIUM & HEART DISEASE • They were also associated with a smaller, nonsignificant increase in the risk of stroke and mortality • Based on the data analysis, treatment of 1000 people with Ca++ for 5 years would cause an additional: ♥ 14 MI ♥ 10 Strokes ♥ 13 Deaths ♥ Prevent 26 fractures 15 Bollard MJ, et al. BMJ 2010;341:c3691
CALCIUM & HEART DISEASE • Coadministration of Ca++ and vitamin D had no effect on the risk of CHD or stroke on the Women’s Health Initiative16 Conclusions • Ca++ supplements without coadministration of vitamin D are associated with an increase incidence of MI 15 Bollard MJ, et al. BMJ 2010;341:c3691 16 Hsia J, et al. Circulation 2007;115:846
VITAMIN D & HEART DISEASE • Low levels of 25-OH D, the principal circulating storage form of vitamin D, are present in 1/3 to 1/2 of healthy middle –aged to elderly adults • Clinical studies have reported associations between lower vitamin D levels and CVD • A study using participants (n=1739) from the Framingham Offspring Cohort (FOC) – 55% women 17 Wang TJ, et al. Circulation 2008;117:503-511
VITAMIN D & HEART DISEASE • The age- and sex-adjusted 5-year rate of CVD was approximately twice as high in those with 25-OH D <15 ng/mL as in those with ≥15 ng/mL (HR 2.04 p<0.001) • This association remained significant after adjustments for conventional CV risk factors and renal function (HR 1.62 p=0.01) 17 Wang TJ, et al. Circulation 2008;117:503-511
VITAMIN D & HEART DISEASE • The higher risk associated with vitamin D deficiency was particularly evident in individuals with HTN with vitamin D levels <15 ng/mL (HR 2.13, p=0.003) Potential Mechanisms • Receptors for vitamin D are expressed in vascular smooth muscle cells, endothelial cells, and cardiomyocytes 17 Wang TJ, et al. Circulation 2008;117:503-511
VITAMIN D & HEART DISEASE • 1,25-OH D directly suppresses renin gene expression – downregulating the renin-angiotensin system • Vitamin D modulates smooth muscle cell proliferation, inflammation, and thrombosis • Vitamin D deficiency triggers secondary hyperparathyroidism • PTH promotes myocyte hypertrophy and vascular remodeling 17 Wang TJ, et al. Circulation 2008;117:503-511
VITAMIN D & HEART DISEASE Conclusions • Vitamin D deficiency is associated with increased CV risk above and beyond established CV risk factors • These data raise the possibility that treatment of vitamin D deficiency could reduce CV risk • However, no RCT are presently available to prove this 17 Wang TJ, et al. Circulation 2008;117:503-511
GUIDELINES UPDATE 2011 Prevention of CVD in Women–Guidelines 201117 • Risk Classification in Women • High risk • New cut point for high risk 10-year risk for all CVD, not just CHD • 10-year risk of ≥10% not 20% CHD CVA PAD AAA CVD DM End-stage CKD 10-year predicted risk for CVD ≥10% 18 Mosca L, et al. Circulation March 22, 2011
GUIDELINES UPDATE 2011 Prevention of CVD in Women–Guidelines 201117 • Risk Classification in Women • At Risk • Optimal Risk HTN Dyslipidemia Smoking Poor Diet Physical Inactivity Obesity Family Hx of Premature CAD ≥1 major CVD risk factor Metabolic Syndrome Subclinical vascular disease (coronary Ca++) Poor exercise tolerance on treadmill testing Framingham global risk <10% and a healthy lifestyle with no risk factors 18 Mosca L, et al. Circulation March 22, 2011
GUIDELINES UPDATE 2011 • Lifestyle Interventions • Physical Activity 150 min/wk of moderate exercise, 75 min/wk of vigorous exercise, or an equivalent combination. Aerobic activity should be performed in episodes of at least 10 min. Women should be advised that additional CV benefits are provided by increasing activity to 5 hr/wk (300 min/wk) 18 Mosca L, et al. Circulation March 22, 2011
GUIDELINES UPDATE 2011 Unless contraindicated • Preventive Drug Interventions - Aspirin • High-risk Women • At Risk or Healthy Women • Aspirin (75-325 mg/d) should be used in women with CHD (Class I) • Aspirin (75-325 m/d) is reasonable in women with DM (Class IIa) • If high-risk woman has an indication but is intolerant to aspirin, clopidogrel should be instituted (Class I) • Aspirin can be useful in women ≥65 y/o (81 mg/d or 100 mg qod) if BP is controlled & benefit for ischemic stroke & MI prevention is likely to outweigh risk of GI bleeding and hemorrhagic stroke (Class IIa) 18 Mosca L, et al. Circulation March 22, 2011
GUIDELINES UPDATE 2011 • Preventive Drug Interventions • Dabigatran: Atrial Fibrillation Dabigatran is useful as an alternative to warfarin in patients with paroxysmal to permanent atrial fibrillation and risk factors for stroke or systemic embolization who do not have prosthetic valve or hemodynamically significant valve disease, severe renal failure (creatinine clearance 15 mL/min), or advance liver disease 18 Mosca L, et al. Circulation March 22, 2011
WHAT WE WANT OUR PATIENTS TO LOOK LIKE AND TO DO IN THEIR 80s