Download
1 / 19
200 likes | 326 Vues
GLOBAL MAINTENANCE DIALYSIS POPULATION FROM 1990 TO 2010. Others. Glomerulone phrites. 10%. 13%. Diabete s. Hypertension. 50.1%. 27%. D iabetes and Hypertension : The most common causes of ESRD. USA World. No. Of patients. 700. Pro jection. 95% C I. 600. 520 240 2 095 000. 500.

E N D
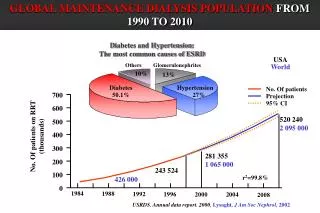
GLOBAL MAINTENANCE DIALYSIS POPULATION FROM 1990 TO 2010 Others Glomerulonephrites 10% 13% Diabetes Hypertension 50.1% 27% Diabetes and Hypertension:The most common causes of ESRD USA World No. Of patients 700 Projection 95% CI 600 520240 2 095 000 500 No. Of patients on RRT (thousands) 400 300 281355 1 065 000 200 243524 100 r2=99.8% 426 000 0 1984 1988 1992 1996 2004 2000 2008 USRDS. Annual data report. 2000, Lysaght, J Am Soc Nephrol, 2002
Hypertension and Diabetes prevalence in the world: the numbers of an epidemic HTN: 1 billion (20-25% of GP) DM: 177 millions (6-7 % of GP) Europe USA HTN: 114 millions DM: 21 millions China HTN: 60 millions DM: 17 millions HTN: 130 millions DM: 19 millions Wolf-Maier K et al. Hypertension 2004; King H, Diab Care 1998
Possible course of renal involvement in type 2 DM Incipient nephropathy Overt nephropathy 160 120 80 40 0 GFR (ml/min • 1.73m2) 2 ml/min/year 4-7 ml/min/year ESRF ~20% 5 10 15 20 25 30 2000 200 20 2 AER (g/min) 5 10 15 20 25 30 progressors non progressors Diabetes duration (years) Mogensen et al., 83, 86, 89, 90
ECF expansion, vasoactive hormones (AII, ET ecc.) HYPERGLYCEMIA HIGH BLOOD PRESSURE AGE formation Polyol pathway PKC TGF-ß, PDGF, TNF- α , iNOS Renal vasodilation synthesis and/or degradation of extracellular matrix Glomerular Glomerular hypertension Mesangial and interstitial matrix Protein Filtration GBM thickness and selectivity GLOMERULOSCLEROSIS TUBULO INTERSTITIAL FIBROSIS
Fattori di rischio per lo sviluppo e la progressione della nefropatia diabetica • scarso controllo glicometabolico • ipertensione sistemica • microalbuminuria o proteinuria • durata del diabete • fattori genetici • Sesso maschile • Predisposizione familiare ad ipertensione, diabete e malattie CV • Predisposizione razziale • Mutazioni in geni candidati • fumo • alterazioni lipidiche • elevato apporto proteico(?) • alterazioni dell’emostatsùsi (?) • iperfiltrazione glomerulare precoce (?)
40 1 p < 0.001 30 A B 20 0.7 C 10 Overall: p < 0.001 0 0 Stroke CAD 0 10 20 30 40 50 60 70 80 90 Months Albuminuria as apredictorof CVD in T2DM A: U-Prot < 150 mg/L B: U-Prot 150–300 mg/L C: U-Prot > 300 mg/L 0.9 0.8 Survival free of CVD Incidence (%) 0.6 0.5 Miettinen H et al. Stroke 1996;27:2033-2039.
Microalbuminuriapredicts the developement ofclinical proteinuria:the MICRO-HOPE Study Ma - Ma + Adjusted O.R. 18(CI 12-27) P< 0.001 Adjusted O.R. 17 (CI 12-24) P< 0.001 Adjusted O.R. 18(CI 12-24) P< 0.001 RISK of PROTEINURIA % All n=7674 DM n=3223 No DM n=4451 Modified from Mann JFE et al., JASN 2003
Algoritmo per lo screening ed il trattamento della microalbuminuria Screening del paziente diabetico per microalbuminuria (ACR) Microalbuminuria confermata in almeno due occasioni Il controllo glicemico è soddisfacente? Ottimizzare il controllo glicemico Controllo glicemico soddisfacente Microalbuminuria confermata in almeno due occasioni Terapia antipertensiva Ace-I o Sartani • Obiettivi • PA < 130/85 mmHg • Riduzione della microalbuminuria Obiettivo non raggiunto Obiettivo raggiunto Titolare la dose di ACE-I o Sartano, considerare altri antipertensivi Trattare i fattori di rischio associati (es. lipidi ecc.) Proseguir eil monitoraggio dell’albuminuria ogni 3-6 mesi
No AHT ACE-I ± Diur. -blockers ± Diur. Triple or Conv.Tx (T) CCB ACE-I + T RELATIONSHIPS BETWEEN MEAN ARTERIAL PRESSURE AND THE RATE OF DECLINE IN GFR IN TYPE 1 PATIENTS WITH NEPHROPATHY (Data sources: 12 studies, 960 patients) 16 12 Decline in GFR (ml/min/yr) 8 4 6,8245 y = 7E-14x R = 0,9996 0 MAP (mmHg) 95 105 115 125 G. Deferrari, 2001
Renal Protection: the importance of RAAS Blockade Type 2 diabetic renal disease patients: meta-analysis Pooled RR= 0.72 (P< 0.001) RRR 28%, NNT 40 N= 3228 patients, 2 studies mean follow-up 2.9 yrs MAP 97 vs 99 7.9% x2 S creat/ 100 pts/ year 6.5 % NON ARB ARB Based on Renaal and IDNT database
The CALM Study CAndesartan and Lisinopril on Microalbuminuria in type II diabetes BP Adjusted ACR reduction at 24 weeks Cand 16 (N= 42) Lis 20 (N= 43) C + L 16 + 20 (n= 46) Percent * † † ‡ *P = 0.05 vs baseline †P < 0.001 vs baseline ‡P = 0.04 vs Candesartan Mogensen CE, BMJ 2000
Linee guida per la prevenzione della microalbuminuria (prevenzione primaria) • Normoalbuminuria e PA<130/80 • Accurato controllo glicemico: HbA1c <7.5% • ACE-inibitori? • Normoalbuminuria e PA>130/80 • Accurato controllo glicemico, correzione dell’eccesso ponderale, riduzione dell’apporto sodico, abolizione del fumo, riduzione dell’apporto di alcool
Linee guida per la prevenzione della nefropatia clinica (prevenzione secondaria) • Accurato controllo glicemico: HbA1c <7.5% • PA ottimale: 120/70-75 se < 50 anni; 125-130/80 se > 50 anni • ACE-I (di scelta nel DM tipo 1), nel DM tipo 2 anche Sartani • Altri antipertensivi da sostituire ai suddetti se poco tollerati: ACE-I, Sartani, Calcio antag. a lento rilascio • Altri antipertensivi eventualmente da associare per raggiungere la PA ottimale: calcio antag., alfa-bloccanti, beta bloccanti, diuretici tiazidici • Dieta iposodica se PA > 130/80 • Controllo della dislipidemia, riduzione del sovrappeso, abolizione del fumo e dell’apporto di alcool • Dieta normoproteica (0.9-1 g/Kg/die)
Linee guida per rallentare la progressione della nefropatia diabetica (prevenzione terziaria) • controllo glicemico? • PA ottimale: 120/75 se < 50 anni; 125-130/80-85 se > 50 anni • ACE-I (di scelta nel DM tipo 1) sartani (di scelta nel DM tipo 2) • Altri antipertensivi da sostituire ai suddetti se poco tollerati: calcio antag. a lento rilascio • Altri antipertensivi utili per raggiungere la PA ottimale: calcio antag., alfa-bloccanti, beta bloccanti, diuretici • Dieta iposodica e riduzione del peso • Controllo della dislipidemia, abolizione del fumo e dell’apporto di alcool • Dieta lievemente ipoproteica (0.7-0.9 g/Kg/die) ed ipofosforica
Multifactorial intervention and CV disease in T2DM Variable RR (C.I.) P Value P= 0.007 Nephropathy 0.39 (0.17-0.87) 0.003 Retinopathy 0.42 (0.21-0.86) 0.02 Aut. Neuropathy 0.37 (0.18-0.79) 0.002 Periph. Neuropathy 1.09 (0.54-2.22) 0.66 Conv. Tx 0 10 20 30 40 50 Int. Tx Primary composite end-point % 1 1.5 2.0 0 24 48 72 96 0.5 0 months N° at risk Int. Tx betterConv. Tx better Conv. Tx Int. Tx 80 70 59 44 19 80 74 66 61 13 Modified from Gaede P et al. N Eng J Med 2003
Effect of interventions to prevent cardiac events in patients with Type 2 Diabetes Mellitus • Events Rate • Events/1000 pers /yr • N° studies Tx / Control • Cholesterol lowering 5 30/41 • - Primary prevention 2 8/19 • - Secondary prevention 3 34/44 • Blood pressure lowering 3 17/23 • Glucose Lowering 2 15/18 Summary rate ratio (95% CI) 1 1.5 2 0 0.5 Favour Tx Favour Control Modified from Huang ES, Am J Med, 2001
Cost effectiveness of various therapeutic interventions in type 2 DM Incremental cost indicates the balance between total cost (cost of treatment + cost of complications) of standard and that of intensive treatment. Modified from the CDC Diabetes cost-effectiveness group, JAMA 2002.
Attuali problemi e controversie nella prevenzione e trattamento della nefropatia diabetica • Gli ACE-I e i Sartani hanno simile efficacia? • Quale è il dosaggio ottimale di ACE-I e Sartani? E’ utile la loro associazione? • ACE-I e Sartani dovrebbero essere prescritti ai diabetici normotesi normoalbuminurici? • Quale è il target pressorio ottimale? • Il monitoraggio dell’albuminuria è un parametro adeguato per valutare la progressione del danno renale?