Download
1 / 58
580 likes | 800 Vues
The Contraceptive Pill in Practice. Dr Helen Dewhirst Bowling Hall Medical Practice 1/4/2009. 1. A 16yr old attends wishing to start the pill. She has no contraindications to COC use. When will you tell her to start and how will you tell her to take it?.

E N D
The Contraceptive Pill in Practice Dr Helen Dewhirst Bowling Hall Medical Practice 1/4/2009
1. A 16yr old attends wishing to start the pill. She has no contraindications to COC use. When will you tell her to start and how will you tell her to take it?
2. A 21yr old attends post partum, wanting the pill again. No contraindications to COC use. When will you tell her to start it? Will she need to use condoms and for how long?
3. An 18 yr old student requests the pill for the first time. She has no contraindications. What will you tell her about the likelihood of failure?
4. A 17yr old, at school, taking her A levels this year, wants reliable contraception. She has acne and is worried the pill will make it worse.
5. A 17yr old, already on the pill, tells you that her older sister has recently been in hospital and has been taking anticoagulants for a leg thrombosis. What will you advise?
6. A 19 yr old on the COC is due for an admission for orthopaedic surgery. What will you advise her about her pills?
7. 21 yr old student , taking microgynon 30 for 18/12. She says that she is now beginning to feel depressed and ‘bloated’. She wants to try another pill. How will you proceed?
8. A 25yr old woman has just had a termination as a result of COC failure. She would like to try the pill again, but is concerned about it failing again. How could you help?
9. A 30yr old woman is on anti-epileptic therapy. She has been using condoms but would now like to try the pill. How would you proceed?
10. A 14yr old who had not started periods but is sexually active cone requesting the pill. How would you proceed?
11. A 48yr old woman has been taking microgynon for the past 18 years and is happy on it. What are you going to discuss with her?
12. A client attends complaining of headache at the time of a period. She is on femodene. The headaches always start two days after stopping the pill and continue until she starts the COC again.
13. A 24 yr old complains of BTB on microgynon 30. What are you going to do?
14. A 15 yr old school girl requests COC to control her period , which are becoming painful.
15. 20 year old developed migraine after starting the COC. She last had migraine two months ago with numbness in her face and speech difficulty. She wants to continue the pill. What are you going to discuss with her?
16. A 22 old dislikes taking Cilest as she thinks they make her feel sick. She has heard about the contraceptive patch and would like to try it. What are you going to advise?
17. 25 yr old woman attends for emergency contraception having forgotten her pill and had UPSI. What would you discuss with her?
1. A 16yr old attends wishing to start the pill. She has no contraindications to COC use. When will you tell her to start and how will you tell her to take it?
Starting regimes • Day 1or 2 of cycle. Then no additional contraception is required. • Day 3 or later on menses, in which case 7 days extra precautions required. • Quick start; This regime allows starting at anytime in cycle PROVIDED that there has not been a conception exposure risk that cycle already. 7 days extra precautions required. This is unlicensed and as such needs discussing and consent from the patient which should be documented.
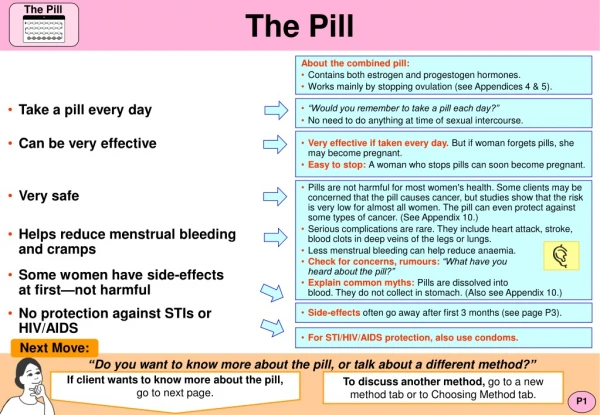
Other important information to impart on first visit • FPA leaflet. Keep for reference • Only works if you take it, each new packet should start on same day of week. • Even if bleeding, keep taking the pills. • Never be late to restart • Only safe in PFI if start the next packet • Late rules • Vomiting/ intercurrentillness • SEs • STI protection • How to get help and advice
2. A 21yr old attends post partum, wanting the pill again. No contraindications to COC use. When will you tell her to start it? Will she need to use condoms and for how long?
Post partum • No lactation, day 21( unless severe pregnancy related hypertension) as ovulation can occur 28 days post partum. No condoms required. • Lactating, not recommended.
3. An 18 yr old student requests the pill for the first time. She has no contraindications. What will you tell her about the likelihood of failure?
Failure rates • Failure rates are described per 100 women years. Perfect usage failure rate is 0.3 per 100wys. Typical use data from USA 8 100wys. • Age social class, acceptability of contraception are factors here.
4. A 17yr old, at school, taking her A levels this year, wants reliable contraception. She has acne and is worried the pill will make it worse.
Acne • An oestrogen dominant COC will help with mild acne, such as marvelon. • Marvelon which contains desogestrel does however have a slightly higher risk of VTE ( due to the fact that it is oestrogen dominant, and this needs to be explained.) • Yasmin is effective for moderate to severe acne. It is drospirenonewith EE. Drospirinoneis antiandrogen as well as having mineralocorticoid activity. • Dianette, cryproteroneand ethyiylestradiolhas not had a head to head with Yasmin, but Yasmin is thought to be as good. Dianette has an increased VTE rate yet to be shown for Yasmin Its duration should be limited due to liver tumour. It should not therefore have a place for a new user.
5. A 17yr old, already on the pill, tells you that her older sister has recently been in hospital and has been taking anticoagulants for a leg thrombosis. What will you advise?
VTE • Need to establish whether her sister ( can assume under 45yrs) had precipitating risk factors for a VTE, eg surgery or post partum, and whether a clotting screen has been carried out and results available. • WHO 4; FH Factor V Leiden, • WHO 3; FH thrombosis ,clotting screen not available no ppts , • WHO 2; FH with no ppt and NORMAL clotting. • These categoroes of risk need to be discussed further.
6. A 19 yr old on the COC is due for an admission for orthopaedic surgery. What will you advise her about her pills?
Surgery • Risk is for major surgery or leg surgery. • To stop from at least 2 weeks prior ( best 4 weeks) until 2 weeks afterward.
7. 21 yr old student , taking microgynon 30 for 18/12. She says that she is now beginning to feel depressed and ‘bloated’. She wants to try another pill. How will you proceed?
Side effects • Cyclical ‘bloating’ is usually an oestrogen dominant symptom. Microgynon 30 is progesterone a dominant pill. A switch to Yasmin may be helpful here due to mineralocorticoid activity. Depression is a progesterone dominant symptom, so the presence of this would again support the use of Yasmin. Inc risk of VTE to be discussed, and to check not in fact increased BMI. Obviously as good GP will look for and screen for other risk factors for mood disturbance.
8. A 25yr old woman has just had a termination as a result of COC failure. She would like to try the pill again, but is concerned about it failing again. How could you help?
Failure of COC • Many women miss the odd pill, so it would suggest that she is in the 1/5 of women whose ovaries show greater return to activity during the PFI. She could therefore tricycle her pills, taking 3-4 packets back to back and reducing her PFI to 4 days. Some women take a short PFI when BTB occurs. This method means a greater annual consumption of EE than with normal regimes. It is off license. Work is being undertaken looking at taking Loestrin 20 continuously. This has lower annual EE than with regular pill taking. Again off licence.
9. A 30yr old woman is on anti-epileptic therapy. She has been using condoms but would now like to try the pill. How would you proceed?
Enzyme inducers • COC is WHO 3 for women on long term enzyme inducers. If they are chosen they require to take 50ug EE. One brand available in UK, Norinyl 1. FPA guidance is to use 2 microgynon, or femodene and a femodette. This is off licence and named patient. • Benefit from tricycling to maintain a steady hormone state which also helps with the control.
10. A 14yr old who had not started periods but is sexually active cone requesting the pill. How would you proceed?
Amenorrhoea • Assuming she is Fraser competent and there are no child protection issues to resolve a COC is contraindicated in Primary amenorrhea. She should use condoms and not start hormonal contraception until menses occur.
11. A 48yr old woman has been taking microgynon for the past 18 years and is happy on it. What are you going to discuss with her?
Age • WHO 2 In healthy , migraine free, women who have never smoked, age 35-51 . • WHO 3 if ex smokers. However BMI is an independent risk factor. BMI needs to be below 25. • Would be appropriate to suggest switching to a 20ug EE pill , egLoestrin 20, femodette or mercilon.
12. A client attends complaining of headache at the time of a period. She is on femodene. The headaches always start two days after stopping the pill and continue until she starts the COC again.
Mood changes • Important to exclude severe or unusual headache or migraine with aura. As these occur regularly in the PFI, she may benefit from a tricycling regime.
13. A 24 yr old complains of BTB on microgynon 30. What are you going to do?
BTB • Exclude other causes, • a. disease, STI in our population • b. disorder of pregnancy • c. default, missed pills. • d. drugs, enzyme inducers • e. diarrhoea/vomiting • f. duration of use too short. • g. dose
BTB • Reassure, the dosages to maintain endometrium is lower than that required to suppress ovulation. An alternative progesterone may solve the problem, maybe higher dosage, or a bi/triphasic preparation which will have an increasing dosage of progesterone n second half of the cycle.
14. A 15 yr old school girl requests COC to control her period , which are becoming painful.
Other Benefits • The COC is effective in treating dysmenorrhea. It is an unlicensed indication and therefore the risk benefit profile is altered.
15. 20 year old developed migraine after starting the COC. She last had migraine two months ago with numbness in her face and speech difficulty. She wants to continue the pill. What are you going to discuss with her?
Migraine • Did you feel nauseated or sick to your stomach? • Were you bothered by the light a lot more than when you don’t have a headache? • Your headaches limited your ability to work, study or do what you needed to do for at least 1 day?