
OSTEOCHONDROMA
OSTEOCHONDROMA. Cartilage capped exostosis Commonest benign tumour of bone Metaphyseal developmental abnormality. INCIDENCE. 45 % of benign bony tumours 12 % of all bony tumours Become evident < 20 yrs Solitary or multiple Any enchondral ossification bone. CLINICALLY.

OSTEOCHONDROMA
E N D
Presentation Transcript
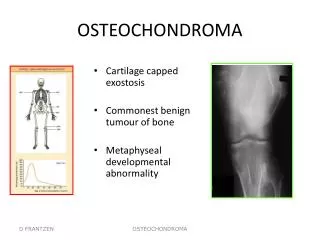
OSTEOCHONDROMA • Cartilage capped exostosis • Commonest benign tumour of bone • Metaphyseal developmental abnormality OSTEOCHONDROMA
INCIDENCE • 45 % of benign bony tumours • 12 % of all bony tumours • Become evident < 20 yrs • Solitary or multiple • Any enchondral ossification bone OSTEOCHONDROMA
CLINICALLY • Lump or mechanical problem • Tendon or nerve irritation • Sessile or pedunculated • 50% distal femur, proximal tibia, proximal humerus OSTEOCHONDROMA
CLINICAL • Active growth during puberty • Move towards diaphysis during growth • Excise if troublesome in second decade OSTEOCHONDROMA
RADIOLOGY • Flat/ sessile / pedunculated • Tumour blending into metaphysis • Pedunculated orientated proximally • Cartilage cap with calcification OSTEOCHONDROMA
PATHOLOGY • Normal bone covered by normal cartilage cap • Cartilage cap resembles normal growth plate • Cartilage more disorganized OSTEOCHONDROMA
PATHOLOGY • Covered by thin layer of periosteum • Binucleate chondrocytes in lacunae OSTEOCHONDROMA
TREATMENT • Nil required unless symptomatic • Extra-capsular marginal excision • Recurrence < 5% OSTEOCHONDROMA
PROGNOSIS • Risk of malignancy if solitary - 0.2 % • Risk of malignancy in diaphyseal aclasia : - 20 % • Sarcomatous changes usually low- grade OSTEOCHONDROMA