
Comparative Analysis of Substance Use Severity in Co-Occurring Disorders
Explore the impact of categorizing psychiatric severity on substance use behaviors and treatment outcomes in individuals with co-occurring disorders. Discover associations between symptom severity levels and substance abuse patterns.

Comparative Analysis of Substance Use Severity in Co-Occurring Disorders
E N D
Presentation Transcript
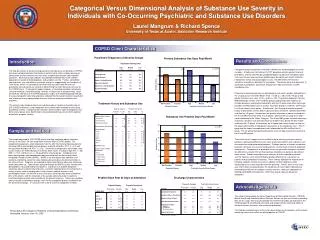
Categorical Versus Dimensional Analysis of Substance Use Severity in Individuals with Co-Occurring Psychiatric and Substance Use Disorders Laurel Mangrum & Richard Spence University of Texas at Austin, Addiction Research Institute COPSD Client Characteristics Psychiatric Diagnoses of Severity Groups Primary Substance Use Days Past Month Results and Conclusions Introduction • Categorical group comparisons revealed no differences on demographic or social variables. At admission to treatment, N-PSY group presented a greater history of prior detox, whereas the PSY group reported higher incidence of emergency room visits over the past year and more problem days during the past month related to employment, family, and psychological issues. No differences were found in substance use patterns between the two groups. The groups were also equivalent at discharge in completion, abstinence, employment, legal involvement, and AA attendance rates. • Dimensional group comparisons on demographic and social variables indicated that the LO group was more often White (X2(6) = 12.66, p < .05) and the HI group had greater homelessness rates (X2(2) = 6.59, p < .05). Psychiatric diagnoses from the MINI differed by severity; the HI and MD groups displayed greater incidence of multiple diagnoses and psychotic disorders and the LO group more often had single disorders of either depression or anxiety. Psychotic disorders, however, were found in all three severity level groups. At admission, the HI group presented a greater history of prior detox and non-detox substance abuse treatment, followed by the MD and then the LO group. Comparisons on primary substance of abuse revealed that the HI and MD were more likely to use opiates, whereas the LO group more often used substances in the “Other” category. The HI and MD groups reported more days of primary substance use and substance use problem days during the past month relative to the LO group. At discharge, the HI group had shorter lengths of stay but the groups did not differ in completion, abstinence, or AA attendance rates. The HI group had the largest unemployment rate, followed by the MD and then the LO group. The LO group had significantly greater levels of legal involvement relative to the HI and MD groups. • The current results suggest that the method used to classify psychiatric severity produces significantly different results when examining relations with substance use characteristics and psychosocial problems. Findings indicate a stronger association between substance use severity and psychiatric severity levels relative to diagnostic comparisons. Comparisons of psychotic versus non-psychotic categories revealed few differences, despite the fact that psychotic disorders are generally considered more severe. Groups formed by cluster analyses of client-reported psychiatric severity, however, were found to display greater differences in substance use patterns and psychosocial functioning. These findings highlight the importance of including symptom severity measures in addition to client diagnoses when conducting assessments to guide treatment planning. Further, these results may also inform efforts to operationalize the Quadrants of Care model, indicating that standardized measures of symptom severity may be a necessary component in defining comorbidity characteristics rather than relying solely on diagnostic categories. The high prevalence of co-occurring psychiatric and substance use disorders (COPSD) has been well documented in the literature and has led to further studies focusing on identification of client features that may affect symptom presentation and treatment outcomes. Research to date indicates considerable heterogeneity in the COPSD population in relation to both diagnoses and symptom severity. Further, comorbidity characteristics may also differ by treatment setting, as suggested by the Quadrants of Care model, which is a conceptual framework that considers both the levels of psychiatric and substance use severity in determining the most likely locus of care for the COPSD client. The quadrant model, however, is theoretical and does not provide concrete methods of operationalizing “severity” of either type of symptomology. Given the diversity inherent in the COPSD population, studies are needed exploring methods of assessing specific client characteristics and potential interactions between psychiatric and substance use symptomatology that may influence clinical presentation and outcomes. The current study compares client and substance abuse treatment characteristics of 215 COPSD individuals using categorical versus dimensional methods of classifying psychiatric severity. Categorical classifications were based on types of diagnoses and dimensional groups were determined using standardized measures of client-reported psychiatric symptom severity. Treatment History and Substance Use Substance Use Problem Days Past Month Sample and Method The sample consisted of 215 COPSD clients receiving substance abuse treatment services in the Texas Co-Occurring State Incentive Grant (COSIG) project. For categorical comparisons, client diagnoses from the Mini International Neuropsychiatric Interview (MINI) were divided into two groups; psychotic disorders (PSY; n = 42) and non-psychotic disorders (N-PSY; n = 173). Dimensional comparisons were made using cluster analysis on 9 Brief Symptom Inventory (BSI) scales, resulting in high (HI; n = 60), (MD; n = 112), and low (LO; n = 43) psychiatric severity groups. Categorical and dimensional groups were compared on data extracted from the Behavioral Health Integrated Provider System (BHIPS). BHIPS is the mandatory data collection and outcomes monitoring system for state-funded substance abuse treatment providers in the state of Texas. Programs are required to report client data at admission, discharge, and 60-day follow-up. Types of data collected through the BHIPS system include client demographics, drug and alcohol use patterns, substance use disorder diagnoses, substance abuse treatment characteristics, and client-reported levels of functioning in a variety of areas such as employment, living situation, medical concerns, and psychological health. At the time of these analyses, discharge data were available for 80% of the clients, with the remainder of the sample continuing to be in treatment. Insufficient follow-up data were available for the present analyses. Continuous variables were analyzed using between-groups t-tests for the categorical groups and ANOVA for the dimensional groups. X2 analyses were used to examine categorical variables. Problem Days Past 30 Days at Admission Discharge Characteristics Acknowledgements The authors acknowledge the Texas Department of State Health Services (TDSHS), Mental Health and Substance Abuse Services Division for their assistance in providing data for this study. We also acknowledge the treatment providers participating in the COSIG project for contributing client data and recognize their continuing efforts to enhance services for clients with co-occurring disorders. The findings and conclusions of this in this presentation are the opinions of the authors and do not necessarily reflect the official position of TDSHS. Presented at the College on Problems of Drug Dependence Conference, Scottsdale, Arizona, June 19, 2006





