Download
1 / 45
450 likes | 662 Vues
IRPA13 Refresher Course RC10 Tuesday 15 th May 2012 Radiation Protection Issues for Novel Radionuclide Therapies Staff Protection and Patient Protection Wendy Waddington Head of Nuclear Medicine Physics Institute of Nuclear Medicine UCL Hospitals NHS Foundation Trust London

E N D
IRPA13 Refresher Course RC10 Tuesday 15th May 2012 Radiation Protection Issues for Novel Radionuclide Therapies Staff Protection and Patient Protection Wendy Waddington Head of Nuclear Medicine Physics Institute of Nuclear Medicine UCL Hospitals NHS Foundation Trust London wendy.waddington@uclh.nhs.uk
History of Radionuclide Therapy History of radionuclide therapy as old as diagnostic nuclear medicine : 32P used to treat leukaemia in 1930’s; still used to treat PRV 131I-Iodide used to treat benign thyroid disease since 1940’s 89Sr chloride, 131I-mIBG, Mab therapy since 1980’s at least
131-Iodide for Benign Thyroid Disease 131Iodine as sodium iodide (NaI) – capsule or oral liquid Stable iodine content very low - can be given to patients with I sensitivity Well established treatment Used for diffuse or nodular toxic goitre, hyperthyroidism, or large NTG EANM Guidelines 2011 www.eanm.org for example Typically administered on outpatient basis in UK 400 / 600 / 800 MBq typically administered
131-Iodide for Benign Thyroid Disease Outpatient therapy : Risk assessment to identify patient-specific risk factors to others → detailed, tailored written instructions to patient and family NaI is excreted in urine, also faeces (limited), also saliva, sweat Comforter and carer consent required if in close contact
131-Iodide for Benign Thyroid Disease Pregnancy/breastfeeding status must be –ve Avoid conception for 4-6 months; male and female Significant issue with respect to travel – Detection of in-vivo activity, even now >12mo possible Patients need to travel with documentation issued at appointment Also carry card identifying patient as receiving 131I for 6 months Required in the event of medical emergency etc.
131-Iodide for Benign Thyroid Disease Treatment of children with Graves Disease if necessary, but only 5-15 yrs Children < 5yr significantly increased risk thyroid cancer Little if any evidence of increased risk in adults 400 or 600 or 800 MBq fixed activity typically administered in UK Empirical; limited evidence base for choice
131-Iodide for Benign Thyroid Disease Dosimetry to achieve optimal response – A contentious issue; practice varies widely Advocated by some; esp. for patients <45 yr 100-150 Gy for TG or NTG, 300-400 Gy for nodular, 150-300 Gy Graves Requires knowledge of thyroid volume (US) and 24 hr % uptake Stunning if pre-treatment 131-I administered ?
131-Iodide for Differentiated Thyroid Cancer 131Iodine as NaI – capsule or oral liquid Again very well established EANM Guidelines 2008 www.eanm.org for example For iodine avid follicular and papillary thyroid ca. Not medullary TC Management is surgery to excise tumour, but residual cells remain : 131Iodide admin for ‘ablation’ of remaining tissue Malignant tissue in thyroid bed and metastases WB scintigraphy + thyroid SPECT/CT @ 7 d post-therapy shows all sites
131-Iodide for Differentiated Thyroid Cancer First adult administration traditionally 3.7 GBq 100 mCi Can range from 1.1 - 5 GBq Low iodine diet for 4-6 weeks prior to admin Repeat admin until no iodine uptake demonstrated Paediatric DTC : Can use 24hr % : <5% 50 MBq/kg, 5-10% 25 MBq/kg, 10-20% 15 MBq/kg Common side effects : Sialadenitis (inflammation of salivary glands) Transient gastritis
131-Iodide for Differentiated Thyroid Cancer Delivered in inpatient setting – Admission for 2d - 1 wk typical Pregnancy/breastfeeding –ve Avoid conception 6-12 months M/F Radiation safety management on discharge similar to benign disease : Risk assessment → Written instructions → Comforter/carers Travel → 12mo+ Carry documentation issued at appointment Carry 131I patient ID card
131-Iodide for Differentiated Thyroid Cancer Dosimetry : Aim to deliver 300 Gy to remnant or 80 Gy to tumour deposits Or 2 Gy to blood, to prevent myelotoxicity Thyroid dosimetry: à and mtissue required, so multiple imaging to 96 hr required mtissueproblematic; and accurate à not much less so 124I PET holds some promise? Blood-based dosimetry – e.g. modified Benua-Leeper model : serial blood sampling + serial whole body counting for % activity
131-Iodide in Thyroid Ca – HiLo trial NEW Traditionally 3.7 GBq administered, but can range from 1.1 - 5 GBq Recent CRUK multicentre trial – HiLo Trial Results now published - NEJM 2012 366(18):1674-85 Impetus - improved primary surgery 3.7 GBq vs. 1.1 GBq - for low risk DTC pts without mets c.400 patients randomised – comparable success rates Potential for o/p therapy ? Certainly reduced dose to patient, and family Next planned trial : 1.1 GBq vs. none
32-P for Polycythemia Rubra Vera For refractory PRV or essential thrombocythemia Occurs generally in later life : 50-70 yr Myeloproliferative disorders → over-production of rbc Suppress by irradiation of bone marrow : 32P incorporates into DNA Well established therapy; over 30 yr EANM Guidelines 2007 www.eanm.org 32P as orthophosphate : PO4 3- orally or by i.v. injection 74–111 MBq by BSA, more as req. max 185–260 MBq / i.v. Or, fixed 111 MBq and if good response not seen, repeat +25% until
32-P for Polycythemia Rubra Vera Outpatient therapy in UK Instructions to patient and family – urinary excretion for 2 d Avoid conception for 4 months Acute risk : leukopenia and thrombocytopenia 4-6 wk Late risk : increased incidence leukaemia – 2-15% at 10 yr Chemotherapy now favoured, use of 32P diminishing High energy beta emitter Essential to shield with perspex during dispensing and injection
Metastatic Bone Pain Palliation Bone metastases experienced by about 30% cancer patients Many therapeutic measures – RN therapy when others fail Bone mets → soft tissue growth into bone cells – osteoblastic reaction Use bone-seeking agents with prolonged retention Also applications in primary osteosarcoma Blood cell count and renal function are considerations Current radiopharmaceuticals; ß emitters - some with weak γ(imaging) : 89Strontium Chloride 150 MBq 153Samarium EDTMP 37 MBq / kg 186Rhenium HEDP 1295 MBq
Metastatic Bone Pain Palliation Administer by direct i.v. inj - slow infusion - avoid extravasation - waste Outpatient therapy, but keep in for 4-6 hr following i.v. – urinary excretion Instruct patient, esp. re hygienic precautions wrt urine incontinence? 89Strontium Chloride longer to respond, longer acting 153Samarium EDTMP more rapid response, shorter duration 186Rhenium HEDP more rapid response, shorter duration
Metastatic Bone Pain Palliation RECENT Alpha emitter 223Radium chloride – rapid uptake bone seeking Ca mimic Developed by Algeta ASA (Norway), with Beyer 223Ra α 11.4 d→ 219Rn α 3.96s → 215Po α 1.78 ms → 211Pb ß 36.1m → 211Bi α 2.17m → 207Tl ß 4.77m → 207Pb stable Recent Phase III clinical trial : reported 2011 – ALSYMPCA - ca. prostate Interim results → 3 mo increase in survival → Trial stopped early Administer 50 kBq / kg by i.v. injection; every 4 weeks for 4-6 mo
Radio Synovectomy Treat joint synovitis – inflammation of connective tissue - beta emitter - Eß Direct intra-articular injection, suitable chemical form, > 10nm particle size 90Yttrium silicate 185 - 222 MBq knee only 186Rhenium sulphide 37, 74, 111, 185 MBq many joints 169Erbium citrate 10, 20, 30, 40 MBq small extremity joints
90-Yttriumlabelled Microspheres For inoperable primary liver cancer (mainly HCC), also liver metastases Direct administration into the hepatic artery via catheter, under fluoroscopy Must aim to inject into the tumour 90Yttrium labelled inert microspheres : SIR–Spheres Sirtex, Australia TheraSphere MDS Nordion, Canada Therapy must be planned – assess pulmonary and gastrointestinal shunting
90-Yttriumlabelled Microspheres Image distribution of 99mTc MAA injected via catheter at planned site Lung shunt fraction (lung activity / lung + liver activity) by planar count data Very inaccurate unless AC, and SC, performed SPECT/CT to assess GI shunting and distribution within liver SIR-Spheres - administer if LSF < 20%; reduce activity if > 10% SIR–Spheres 20-60 um resin 40-80 million 40-70 Bq / sphere TheraSphere 20-30 um glass 1-8 million 2500 Bq / sphere SIR–Spheres 2 - 3 GBq 10-20 ml moderate embolism TheraSphere 3 – 20 GBq 20-60 ml mild embolism Image to confirm distribution – bremsstrahlung GC or 90Y PET
131-Iodine labelled Lipiodol Also for direct intra-arterial administration, for primary liver cancer Lipiodol is (naturally occurring) poppy-seed oil, rich in iodine Lipiocis IBA Belgium Viscous oil, difficult to inject due to resistance Inject slowly through catheter in hepatic artery under fluoroscopic control Lipiodol can melt some plastic syringes, taps etc. CAUTION 2.22 GBq - estimated mean liver dose around 50 Gy Written instructions to patient – esp. re. urinary excretion Image to confirm distribution – SPECT Note Lipiodol is visible on CT
131-Iodine labelled mIBG in neuroendocrine tumours mIBG : meta-iodobenzylguanidine Noradrenaline analogue – taken up in range of neuroectodermal tumours includes neuroendocrine tumours manifested in adulthood : phaeochromocytoma, carcinoid, paraganglioma, medullary thyroid ca and neuroblastoma in infancy and childhood
131-Iodine labelled mIBG in neuroendocrine tumours Treat inoperable, advanced, recurrent, metastatic disease with mIBG Must be inpatient therapy Urinary excretion only (this is not NaI) Written instructions on discharge 131Iodine mIBG available commercially - shipped frozen on dry ice Administer by slow i.v. infusion 3.7 – 11.2 GBq per fraction three fractions typical Co-infusion of anti-emetics Thyroid protection required 14 d
131-Iodine labelled mIBG in neuroblastoma Paediatric neuroblastoma most frequent childhood cancer after leukaemias and brain tumours 50% high risk and often –ve response to chemo, surgery, EBRT Five year survival < 40%, relapse or progression common mIBG also specifically taken up by NB cells – Use 123Iodine mIBG for diagnostic imaging - assess site / avidity uptake 131Iodine for therapy : imaging must be +ve
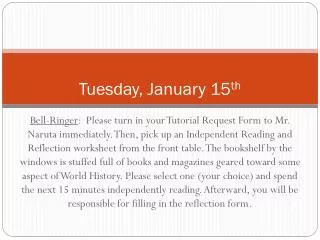
131I-MIBG therapy – metastatic neuroblastoma (stage IV) after 19 GBq 131I-MIBG + 2 weeks before therapy
131-Iodine labelled mIBG in neuroblastoma Typically 3.7 GBq given, now higher activities proven Whole body dose > 2 Gy myeloablative → follow with stem cell transplant UCLH (MATIN) protocol - co-administer Topotecan as radiosensitiser First fraction - 444 MBq / kg 131Iodine mIBG Determine whole body retention with GM counting system in I/P room Get à from WB curve → activity for 2nd fraction (+14 d) to give 4 Gy to WB Can give very high activities – empirically capped at 30 Gy wrt RP Significant potential risk to staff administering Good administration protocol, shielding and training are essential Dosimetry for tumour, kidneys, spinal cord etc. can be helpful
131-Iodine labelled mIBG in neuroblastoma MATIN protocol at UCLH : mIBG to 4 Gy WB dose + topotecan Can lead to very high activities – empirically capped at 30 Gy wrt RP Inpatient therapy → paediatric nursing and medical (oncology) staff Some patients very young < 2 yrs - Comforters and carers essential Carefully explain and counsel C/C Ensure appropriate C/C – not uncommon for mother to be pregnant, or If not yet potty trained then nappies will hold urinary excretion Behavioural restrictions on discharge – esp. wrt siblings, ++ under 5
Radiolabelled Somatostatin Receptor Therapy Neuroendocrine tumours also express somatostatin receptors (SSR) Many analogues developed for radiolabelling : Octreotide (as in 111In Octreoscan for imaging) newer - DOTA-TOC, DOTA-TATE, DOTA-NOC… Choice of analogue also wrt pattern of SSR sub-types in tumour type Choice of radiolabel based on : ßenergy wrt cell range, pattern of cell kill half-life compatible with kinetics of uptake/retention 90Yttrium DOTATATE, 177Lutetium DOTATATE currently most used Both must be labelled in-house - QC, shielding and training essential
Radiolabelled SSR Therapy 90Yttrium DOTATATE used for adult NETs 177Lutetium DOTATATE for NETs, and more recently neuroblastomas 7.4 GBq standard activity prescribed x 4 fractions at 8-week intervals Urinary excretion leads to high renal dose – co-administer amino acids Dosimetry helpful, esp. in neuroblastoma
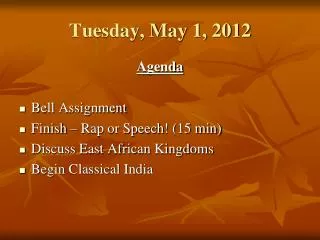
177Lu DOTATATE patient with neuroendocrine pancreatic tumour Post fraction 1 (Top) Post fraction 3 (Bottom) 177Lu DOTA-TATE patient with gastrinoma, partial remission 7.4 GBq x 4 administrations
Radioimmunotherapy Radioimmunotherapy –therapy with radiolabelled Molecular Antibodies Initial work with Mabs, little success with some exceptions, Bivalent Mabs – 2-step admin Recent developments with anti CD20, 22, 45, 66 Mabs for haematological cancers - leukaemias and lymphomas
90-Yttrium ibritumomab tiuxetan (Zevalin) Rituximab - non-active form of anti CD20 Mab ibritumomab – used extensively for non-Hodgkin´s lymphoma Zevalin : treatment of adults with rituximab-relapsed or -refractory follicular B-cell NHL i.e. NOT first-line treatment Approved in Europe 2004 Pretherapy imaging and/or dosimetry with 111In Mab not mandated 90Y beta energy → path length of 100-200 cells → crossfire High retention – 7% urinary excretion
90-Yttrium ibritumomab tiuxetan (Zevalin) Pre-target with unlabelled Mab (Rituximab) as part of treatment Zevalin biodistribution then more favourable - peripheral B-cells cleared Rituximab stops Zevalin binding to non-tumour sites Rituximab also induces tumour cell killing and direct apoptosis Above biological effects + radiation thought synergistic Label in-house, stable for < 8 hours Pharmacy training, QC, adequate beta shielding for labelling essential Administered as slow i.v. infusion with Rituximab over 10 mins 15 MBq / kg upto 1200 MBq Treatment possible as outpatient, patient to be observed for 20-30 min Written instructions re urinary hygiene and contact restrictions
131-Iodine Tositumomab (Bexxar) 131Iodine Tositumomab (Bexxar) anti CD20 Mab GlaxoSmithKline US only Treatment of relapsed or refractory low grade follicular or transformed NHL including rituximab-refractory NHL i.e. NOT first-line treatment Thyroid protection required for 14 d Pretherapy biodistribution + WB dosimetry study mandated – image d0, 4, 7 Cold tositumomab co-infused with 131I pre-labelled tositumomab 185 MBq Calculate activity to delivery 0.75 Gy whole body dose Give tositumomab and x GBq 131I pre-labelled tositumomab 60 ml 20min Inpatient procedure – instructions to patient on discharge
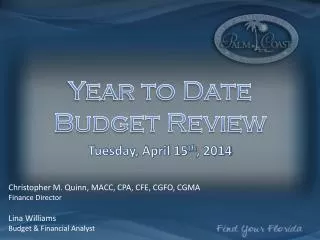
Filter Saline Saline Bag Air filter Syringe filter Syringe 3-way tap 3-way tap Syringe Burette clamp N61 therapy vial connectors Infusion pump To vial To vial To vial Infusion pump To patient
Clinical Management – Some RP Issues Pregnancy / breastfeeding must be excluded – test for pregnancy Conception avoided in M&F, with clear advice from 4-12 mo Patient must be self-caring (risk assess) and able to tolerate isolation Patient prognosis – life expectancy must be predicted > 4 weeks min. Contingency plans for emergency transfers / surgery / unexpected sudden death – incl. out of hours Specialist therapy → regional / national referrals → good handover Inpatient therapy ? Discharge to home, or hotel before home ? Outpatient ? Overnight in patient’s hostel or hotel ? Paediatric ? Comforter Carer support – appropriate C/C Siblings …
Acknowledgements Nuclear Medicine Physicians : Jamshed Bomanji, Peter Ell, Rizwan Syed Oncologists : Mark Gaze, Jenny Gains, Anna Cassoni Clinical Physicists : Matt Aldridge, Therese Soderlund Radiopharmacists : Dominic Lui, Jenny Wootten, Mark Moran Dosimetry Physics : Alan Green, Glenn Flux, Manuel Bardies Matt Guy, Mike Stabin RPAs : Peter Marsden, Mike Short Regulators : Adrian Bush