Download
1 / 51
510 likes | 548 Vues
Future of Disease Management Under CDHC. Tomás D. Valdivia, MD, MS Chief Medical Officer Definity Health. Overview. CDHC introduced new dynamics between the consumer and plan, doctor and DM.

E N D
Future of Disease Management Under CDHC Tomás D. Valdivia, MD, MS Chief Medical Officer Definity Health
Overview • CDHC introduced new dynamics between the consumer and plan, doctor and DM. • IOM and many others are driving toward a patient-centered health care system with ubiquitous information about the system. • “DM” has a unique challenge to respond to the new health care environment to create and support health care consumers.
Agenda • Define Consumer-Drive Health Care • Describe the effect on constituents • Other important activities • Implications for Disease Management
Consumer Driven Healthcare • As a benefit strategy: reduces waste and improves healthcare outcomes (including member satisfaction) by giving members the financial responsibility, information, and tools to become empowered consumers of discretionary and routine healthcare services
Managed care has funded first dollar coverage First dollar coverage works poorly inside an insurance economic model Definity created a tax-effective way to offer a new financial services product for healthcare Unbundled and repackaged the “good stuff” of managed care Consumer Driven Healthcare RAND
CDHC Personal Care Account HealthCoverage Tools andResources 1 2 3 = + + Account Based CDHC Products • Three components that work together to create a consumer driven product • Involved • Informed • Better decisions • Benefit dollars • Rollover feature • No copays • No cash-out opportunity • Comprehensive coverage • Preventive care covered first dollar • Care support and coaching • Personal website • Information on Providers, Treatments, Pricing
CDHC An Example • Meet Phil and Nancy, a growing family with one child, Lisa. Phil and Nancy’s family plan: • Employer-funded PCA allocation: $2,000 • Health Coverage annual deductible: $3,000
Preventive care Physical Exam $ 400Paid by Health Coverage HealthCoverage100% / 70% Non-preventive care Prescriptions (10) $ 400 Urgent care visits (3) 200 Physician’s visits (5) 300 Physical therapy1 (8) 500 Total $ 1,400 Member Responsibility $1,000 Preventive Care Paid by PCA $ 1,400 PCA $2,000 $1,400 Expenses Ded. $3,000 Rollover To Year Two $ 600 Phil and Nancy’s Family Plan—Year One Expenses $600 Rollover 1 May not apply against Health Coverage annual deductible.
Member responsibility Reduced to $400 due to rollover from year one HealthCoverage100% / 70% PCA balance $2,000 employer-funded PCA contribution plus $600 rollover from year one $400 Preventive Care $600 Rollover PCA $2,600 PCA $2,000 Ded. $3,000 Phil and Nancy’s Family Plan—Year Two
Preventive care Physical Exam $ 350Paid by Health Coverage HealthCoverage100% / 70% Non-preventive care Prescriptions (8) $ 350 Lab work 250 Physician’s visits (7) 400 Physical therapy1 (8) 500 Total $ 1,500 $400 Preventive Care PCA $2,600 Paid by PCA $ 1,500 $1,500 Expenses Ded. $3,000 Rollover To Year Two $ 1,100 Phil and Nancy’s Family Plan—Year Two Expenses $1,100 Rollover 1 May not apply against Health Coverage annual deductible.
Member responsibility Reduced to $0 due to rollover from year two HealthCoverage100% / 70% PCA balance $2,000 employer-funded PCA contribution plus $1,100 rollover from year two $1,100 Rollover PCA $3,100 Preventive Care PCA $2,000 Ded. $3,000 Phil and Nancy’s Family Plan—Year Three
Defined Contributionversus CDHC • Defined Contribution: • A benefit strategy, not a benefit design • Limit employer financial liability • Shift costs to employee • Benefit design methods • Fixed annual benefit, regardless of need • Increase co-pays, deductibles, or EE contribution
Concerns about CDHC • Positive selection • Cost shifting for sicker members • Erosion of risk pooling
50.00% 45.00% All Eligible Employees, All Plans Definity Health Enrollment 40.00% 35.00% 30.00% % Enrollment 25.00% 20.00% 15.00% 10.00% 5.00% 0.00% 00 - 25 26 - 35 36 - 45 46 - 55 56 + Employee Age Ranges Actual Enrollment Experience
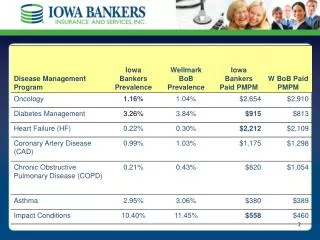
Definity Health Results • Client Satisfaction: 100% renewal • Member Satisfaction: • 97% re-enrollment • 91% satisfaction • Member Web Use: 50% • Care Support Line Use: call volume 70% above benchmark
Utilization Results • Cost control: better than market trend • Utilization: • Inpatient: comparable to M&R well managed • Outpatient: 20% reduction in office visits • Pharmacy: better than Medco tightly managed benchmark • Preventive services: at or above national benchmarks
Measure and Report—Client Plan Comparison 19% decrease in office visits and Rx
Employee Passive Participant Active Consumer Employer PrimaryPurchaser Financial Contributor Health Plan Barrier Enabler Provider Care Manager Restricted New Behaviors
Definition: A Health Care Consumer • A health care consumer is • An individual… • …choosing the services… • …they use… • …and bearing the consequences (financial and others) of those choices. • More technologically savvy • Well-educated • Wealthier than their parents
Our Members: Engaged • Concerned (and informed) about costs • Involved as an active decision maker • Longer term view of healthcare spending • No longer year to year • More interested in preventive health
“Is there a cheaper treatmentthan the one I’m on?” “Which treatment works best?” “Which provider should I see?” Provider Choice “What aboutmy preferences?” “Should I see that provider again?” “What doother peoplethink?” Treatment Choice Whatwill s/he cost? “Does my doctordo a good job?” What Decisions? Plan Choice
Effect on Physicians: Intrigued • Three possible paths: • Continued “commoditization”: price competition only, now at the individual provider level • Differentiation and market segmentation on the basis of quality and value and member preferences • Isolated care monopolies: no change?
Focus on Information Availability • Institute of Medicine -To Err is Human (1999) • Leapfrog Group (2000) • Institute of Medicine - Envisioning the National Health Care Quality Report (2001) • Midwest Business Group on Health - Cost of Poor Quality (2002)
IOM: Quality Chasm Report • Six Aims for Improvement • Safety • Effectiveness • Patient Centeredness • Timeliness • Efficiency • Equity
#2: Care customized to patient needs/values, not professional autonomy #3: Patient is source of control, not the professional #4: Knowledge is shared freely #5: Decision is based on evidence, not training and experience #7: Transparency is necessary IOM: Ten Rules for Redesign
Consumer-Purchaser Disclosure Project (2003) • By January 1, 2007, Americans will be able to select hospitals, physicians, physician groups/delivery systems and treatments based on public reporting of nationally standardized measures for clinical quality, consumer experience, equity and efficiency.
New Directions in DM • Plan Level • Consumer incentives “baked” into the plan • Implicit • Explicit • Plan services integration • Changing perspective: “Right care at the right time, right place,…”
New Directions in DM • Program Features • Consider the practice context at identification step • New information: comprehensible transparency of cost and quality • Support extended to non-standard practices for • value decisions in health care • new transparency of information • non-traditional matters (significant medical decisions) • Create consumers
Geo PPV Built-in incentives Plan svc integration Reach & Engage 2 Measure & Report New perspective Extended support services Evidence packaged for the consumer Educate & Support 3 4 New Directions in DM Identify 1
Better Decisions & Actions Reduced Costs Satisfaction Higher Quality Reduced Costs Higher Quality Satisfaction ER An “Old” New Perspective • Relevant • Complete • Timely • Inexpensive Better Information Consumer Provider
Attributes + Outcomes Cost Value = Provider Choice • Help me find a provider (general). • Is my provider treating me appropriately? • Is there a better provider for me? • Is that provider expensive? • Help me find a provider for this specific problem. A New Perspective Better Decisions & Actions Health Choice • What are my treatment choices? • - Rx-focused • - Procedure-focused • - Disease-focused • What is the right tx for me? • How much should I expect to pay for my care? • How do I stay healthy?
Information – A Personalized Approach • We’ve redefined the member experience • Personalized website • Rich content • Drug bargain finder • Pricing • Quality metrics
Significant Medical Decision Making Health Status improved the same amount over baseline in all three groups JAMA 2002;288:2701 * Statistically significant
Non-traditional Services • Chronic conditions • Diabetes • Asthma • Cardiac • Etc. • Significant medical decisions • Hysterectomy • Low back pain • Cardiac • Etc.
Herniated Disc: In Santa Barbara, CA you are 6× as likely to have surgery then in Bronx, NY. Heart Disease:In Bloomington,IN you are 3× more likely to have bypass than in Albuquerque, NM. Practice Pattern Variation—Geography as Destiny Treatment options: For many problems surgery and medical therapy have equal effectiveness but different side effects.
ABC Co – Discretionary Surgery “Signature” Source: Dartmouth Atlas of Healthcare 1999
What’s the Right Rate? • The “right rate” of healthcare consumption is the rate that results when patients are fully informed and their values and preferences are incorporated into the treatment selection process.