Slide Note
0 likes | 16 Vues
Decreased access to HIV services due to the Anti-Homosexuality Act in Uganda has impacted key populations. PEPFAR-supported programs are adapting to support services for vulnerable groups, although challenges persist. The punitive legislation poses a threat to HIV epidemic control and requires innovative approaches to sustain service delivery.

E N D
Using Client-Centered Models to Sustain HIV Service Delivery to Key Populations in Uganda Vamsi Vasireddy, MD MPH DrPH Country Director, Walter Reed Army Institute of Research, Uganda Ambassador Natalie E Brown US Ambassador to Uganda CAPT Neha Shah, MD MPH Associate Director of Clinical and Laboratory Services, Walter Reed Army Institute of Research, USA The opinions or assertions contained herein are the private views of the author, and are not to be construed as official, or as reflecting true views of the Department of the Army or the Department of Defense.
Summary What is your main question? Courtesy of PinkNews • How can we support uninterrupted HIV services delivery in the face of the latest Anti-homosexuality Act (AHA) in Uganda? What did you find? • Access and utilization of HIV services decreased during the discourse and passing of the AHA, but PEPFAR-supported programs are able to pivot and support services for key and vulnerable populations with partial success. Why is it important? • Punitive legislations targeting key populations have the potential to reverse the gains made towards HIV epidemic control.
The Anti-Homosexuality Act (AHA) of 2023 • Media reporting and public debates on the AHA started in December 2022 and scaled up in January and February 2023. On 21 March 2023, the Parliament of Uganda passed the first draft of the Anti- Homosexuality Act (AHA) and President Museveni ultimately signed the bill into law on 26 May 2023. AHA Criminalizes: • homosexual behavior with sentences ranging from 10 years to life imprisonment. • Promotion of homosexuality, which is undefined and broad enough to include routine public health activities such as HIV prevention, safe sex education, and community engagement. The lack of clarity on “promoting” and “abetting” homosexuality, terms which are ill-defined, creates opportunities for abuse. • Failure to report someone you “suspect” to be violating the AHA, which means everyone in Uganda has a duty to report anyone they suspect to be engaging in homosexual behavior or violating AHA. • Courtesy of Evening Standard • UNCLASSIFIED
Context and Objective • The environment created with the debate and passing of AHA and the associated fear of law enforcement has led to reduced access to KP- focused services. • Understand the effect of the AHA on HIV service provisions and clinic attendance to identify ways to continue to meet needs of KP clients.
PEPFAR and AHA PEPFAR and AHA • The President’s Emergency Plan for AIDS Relief (PEPFAR) the world’s largest assistance program focused on a single disease and supports over 1.3 million people living with HIV on treatment in Uganda. PEPFAR supports 84 drop-in-centers (DIC) across Uganda that provide HIV prevention and treatment services for key population (KP) clients. • Client safety and confidentiality are paramount and only de-identified data is reported from DICs. The DIC names or locations are not disclosed for safety. •
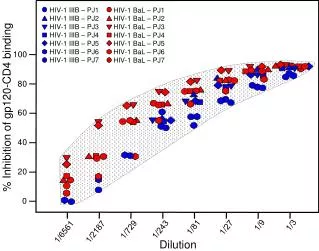
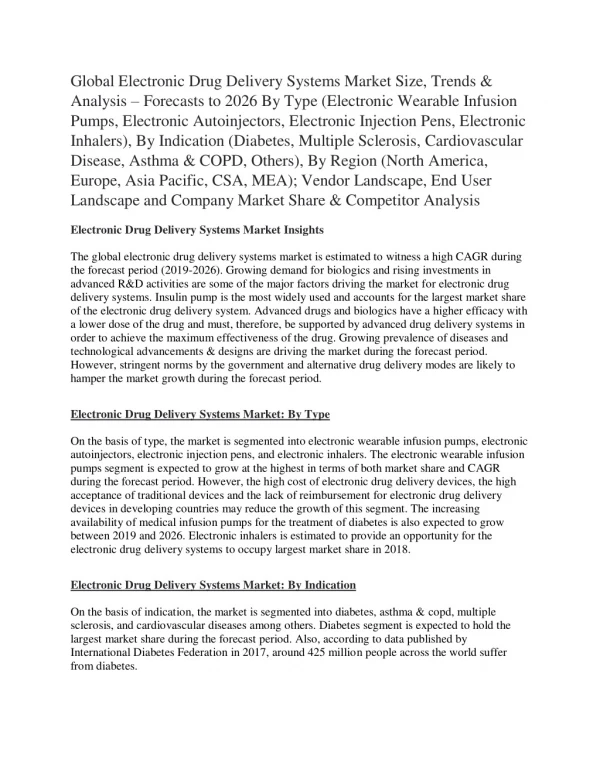
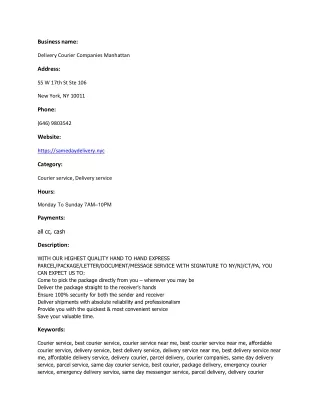
Incidents reported through DICs, Impact and Response; April to June 2023 KP clients targeted by Security Incidents Security Incidents, Distribution 300 80 70 250 60 200 50 150 40 100 30 50 20 0 10 Acholi Ankole East Kampala Lango Masaka Mubende Rwenzori Soroti West_Nile 0 Physical Assault Raids SGBV Arrests 28th-4th May 5th-11th May 12th-18th May 19th-25th May 26th-1st Jun 2nd-8th Evictions Excommunicated Media Outing FSW MSM TG LBQ PWIDs Immediate impact: On going efforts to secure DICs: • Assessments and mitigation plans • Sensitization • Information security training, • Incident reporting and follow up • Planned training in staff and client safety and security Planned strategies to secure KP DICs - Lift Equity • Biometric access • Lockable cabinets • Self-encrypting hard drives • Guards • Cameras • • Reduced client flow at DICs Temporary closure of 4 DICs (FARUG, Freedom, Trans youth initiative and Kuchu shinners) Reduced physical contact by facility staff in communities • Data source: PEPFAR DIC weekly report UNCLASSIFIED
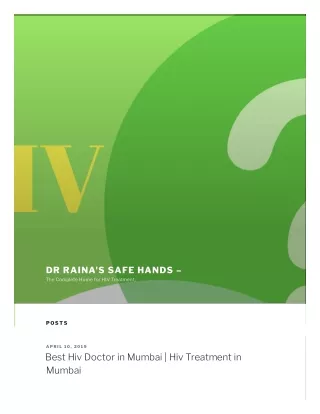
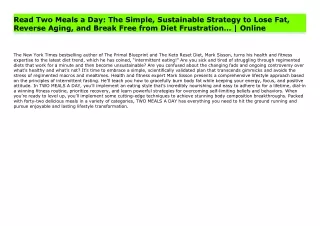
Impact of AHA on select DICs Impact of AHA on select DICs Weekly cumulative service delivery visits at 3 DICs 75 70 65 Media reporting and public debates 60 55 50 Number of clients 45 45 PEPFAR begins adapting 40 AHA debated in the Parliament 36 35 30 28 25 20 16 15 13 10 6 6 5 5 2 0
Impact of AHA on select DICs Chart 2: Weekly cumulative service delivery visits at 3 DICs 75 70 70 65 60 57 55 Number of clients 51 50 49 47 46 45 40 40 AHA in Parliament 37 35 30 26 25 23 20 15 AHA becomes a law 10 6 5 2 0 13-19 Mar 20-25 Mar 26 Mar - 1 Apr 2-8 Apr 9-15 Apr 16-22 Apr 23-29 Apr 1-6May 7-13 May 14-20 May 21-27 May 28 May - 3 June Additional PEPFAR adaptations, monitoring, and consultations support KP clients PEPFAR adaptations continue
Impact of AHA on select DICs Impact of AHA on select DICs – – summary summary Chart 3: Weekly cumulative service delivery visits at 3 DICs 75 70 70 65 64 60 57 55 AHA in Parliament 51 50 Number of clients 49 47 46 45 45 41 40 40 40 37 36 35 30 28 AHA becomes a law 26 25 25 23 20 16 15 13 10 6 6 5 5 2 0 2-8 Jan 9-15 Jan 16-22 Jan 23-29 Jan 30 Jan - 5 Feb 27 Feb - 5 Mar 6-12 Mar 13-19 Mar 20-25 Mar 26 Mar - 1 Apr 2-8 Apr 9-15 Apr 16-22 23-29 Apr 1-6May 7-13 May 14-20 May 21-27 May 28 May - 3 June 4-10 June 11-17 June 18-24 June 25 June - 1 July Apr PEPFAR program adaptations began early Feb and ongoing monitoring, consultations, and adaptations to support KP clients
PEPFAR Adapting to AHA: Innovative KP Programmatic Shifts UNCLASSIFIED
PEPFAR strategies for robust KP programs Structural: Increase the capacity of KP CSOs to advocate, engage and respond to stigma, discrimination and violence • Address the LEA recommendations • Community awareness campaigns on KP rights • KP competency assessments. • Community engagement and capacity building through the national CSO mechanism • Strengthen DIC security Service delivery: Build and strengthen client centered and integrated health services for KP clients • Strengthen service delivery at DIC • Strengthen mental health services. • Roll out virtual interventions • Community-led service delivery through subgrants • Scale up proven DSDM like CRPDDP for PrEP and ART • Evidence-based social protection interventions for KPs • Enhance safety, security, and service access for KP/PP DICs and communities • Institutionalize a multi-sectoral HIV stigma and discrimination (S&D) reduction response • Innovative person-centered telehealth interventions; to ensure HIV service access/continuity LIFT UP Equity Fund ($3M) Roll out new, discreet and long- acting PrEP products • Pilot implementation of CAB-LA targeting 5,000 clients. • Support programmatic implementation (HW training, IEC materials development and dissemination and policy/guidelines update) of the PrEP rings procured by Global Fund. UNCLASSIFIED
Discussion Discussion While select DICs have shown increased utilization of KP-focused services, it is not consistent across the remaining DICs and prone to change with the enforcement of AHA. • PEPFAR programs are resilient and adaptable to rapidly changing circumstances, and support service delivery to key and vulnerable populations as shown by the program adaptations. • Advocacy from global and local stakeholders led to the Ministry of Health issuing a circular stating that all Ugandans should receive health services irrespective of sexual orientation. • However, the AHA supersedes any MOH circular and the fear of being identified and arrested prevents many KP clients from accessing essential health services. This can potentially reverse the gains made towards achieving HIV epidemic control. • The United States government stands in solidarity with the key and vulnerable populations and remains committed to support equitable HIV services without stigma and discrimination. •