
Wanabsorpsie
Wanabsorpsie. Dr. WM Simmonds Internal Medicine (Gastroenterology) 15 August 2011. Wanabsorpsie. Abnormale absorpsie van enkele of veelvuldige nutriente in die gastro-intestinale sisteem. 3 komponente nodig vir optimale absorpsie Intraluminaal WANVERTERING

Wanabsorpsie
E N D
Presentation Transcript
Wanabsorpsie Dr. WM Simmonds Internal Medicine (Gastroenterology) 15 August 2011
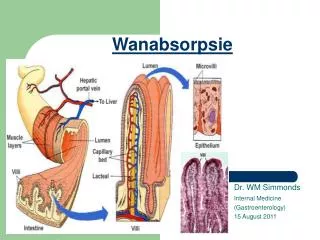
Wanabsorpsie • Abnormale absorpsie van enkele of veelvuldige nutriente in die gastro-intestinale sisteem. • 3 komponente nodig vir optimale absorpsie • Intraluminaal WANVERTERING • Galsuur of pankreas ensiem gebrek • Mukosale WANABSORPSIE • Abnormale mukosa or onvoldoende funksionele derm lengte (‘Brush border surface area’) bv. Dunderm reseksie. • Post-mukosale limfdreinering obstruksie
Malabsorption Syndrome Pallor/Anaemia Night blindness (Vit A) Osteoporosis with pathological fractures Muscle wasting Muscle weakness Tetany (Low Calcium) Hypopigmentation/ Pellagra(Niacin) Ascites (Low Albumin) Dehydration (Diarrhoea) Ecchymoses (Vit K factor deficiency) Steatorrhoea Increased fecal fat Oedema (Low Albumin) Peripheral neuropathy (B12 def) Glossitis, stomatitis Apthous ulcers (Iron & B Vitamin deficiency) Pathological Weight loss
Due to infective agents Intestinal tuberculosis HIV related malabsorption Tropical sprue Parasites e.g. Giardia lamblia. Due to structural defects Inflammatory bowel diseases - Crohn's Disease Fistulae, diverticulae and strictures, Infiltrative conditions - amyloidosis Short bowel syndrome Due to mucosal abnormality Celiac disease Cows' milk intolerance Soya milk intolerance Fructose malabsorption Due to enzyme deficiencies Lactase deficiency Sucrose intolerance Intestinal disaccharidase deficiency Intestinal enteropeptidase deficiency Due to digestive failure Pancreatic insufficiencies: Cystic fibrosis Chronic pancreatitis Pancreas carcinoma Zollinger-Ellison syndrome Bile salt malabsorption Terminal ileal disease Obstructive jaundice Liver cirrhosis Bacterial overgrowth Primary bile acid diarrhea Oorsake van Wanabsorpsie
Celiac siekte • Gluten sensitiewe enteropatie • Algemeen in Europieërs (1:300) • Seldsaam in swart mense • HLA DQ2 en DQ8 • Kan op enige ouderdom presenteer • Gewoonlik - moegheid, gewigsverlies en anemie in ‘n jong/middeljarige dame.
Celiac siekte • Word geasossieer met: • Tipe I diabetes • Tiroid siekte • Addison se siekte (Autoimmuun) • Diagnose: • Anti-endomesiale antiliggame • anti-tTG (weefsel transglutaminase) • Dun derm mukosale biopsie • Vermeerderde intraepiteliale limfosiete • Kript hiperplasia • Villus atrofie
Celiac siekte • Terapie/behandeling • Streng Gluten vrye dieet. Dietkundige belangrik. • Supplemente (FeSo4, Vitamiene) • Behandel osteoporose • Ander geasossierde autoimmuun toestande moet uitgeskakel word. • Goeie opvolg • Klieniese beeld • Antiligame
Kroniese pankreatitisDefinisie • Onomkeerbare pankreatiese skade • Histologiese or radiologiese bewys van kroniese inflammasie en fibrose • Verlies aan eksokrine (asinere selle) en endokriene (eiland selle) pankreas weefsel.
Alcohol and Gallstones most common causes in developed countries (70%) Kroniese pankreatitisOorsake (TIGAR-O) Toxic/Metabolic • Alcohol • Smoking • Hypercalcaemia • Hyperlipidaemia Idiopathic • Early onset • Late onset • Tropical Genetic • Autosomal dominant • Hereditary pancreatitis (PRSS1 mutations) • Autosomal recessive or modifier genes • CFTR mutations • SPINK1 mutations • Others • Autoimmune • Autoimmune pancreatitis • IgG4 related systemic disease • Recurrent • Post Necrotic • Chronic alcoholism • Diabetes Mellitus • Radiotherapy • Obstructive • Benign pancreatic duct obstruction • Gallstones • Stricture • Pancreas divisum • Malignant stricture • Ampullary of duodenal carcinoma • Pancreatic adenocarcinoma
Kroniese pancreatitisPatofisiologie (Alcohol) Alcohol Cytokine release stimulate stellate cells to form collagen (fibrosis) and increase cell - mediated inflammation Chronic Pancreatitis
Jaster, Molecular Cancer. 2004 3:26 doi:10.1186/1476-4598-3-2
Kroniese pankreatitisKliniese einskappe • Ander: • Moegheid, etc • Gewigsverlies agv. wanabsorpsie • Pain geassosieered met hoe proteien and vet iname
Kroniese pankreatitisAbdominale pyn • Most common clinical problem • Decreases appetite and limits food consumption - weight loss and malnutrition • Dramatic reduction in quality of life • Character: • Epigastric, often with radiation to the back. • Boring, deep, and penetrating and is often • Associated with nausea and vomiting. • Relieved by sitting forward or leaning forward, the knee-chest position • Worsens after a meal and often is nocturnal. • Possible causes: • Acute inflammation/noxious stimuli • Increased intra-pancreatic pressure and ischaemia • Neuropathic (Alterations in nociceptive nerves) • Other
Kroniese pankreatitisSteatorrhoea • Exocrine insufficiency. • Passage of bulky, floating, foul-smelling stools or may even note the passage of frank oil droplets. • Occurs when pancreatic lipase secretion is reduced to less than 10% of the maximum output. • A feature of far-advanced chronic pancreatitis or complete blockage of the pancreatic duct.
Kroniese pankreatitisDiabetes Mellitus • Endocrine insufficiency • Half of patients with chronic pancreatitis who develop diabetes will require insulin. • Insulin-producing beta cells and glucagon-producing alpha cells are injured. • Increased risk of prolonged and severe hypoglycemia with over vigorous insulin treatment due to the lack of a compensatory release of glucagon.
Kroniese pankreatitisDiagnose(1) • Kliniese eienskappe (Abdominale pyn, Steatorrhoea, Diabetes Mellitus) • Pankreas funksie toetse • Direk • Direct hormonal stimulation tests are believed to be the most sensitive function test for chronic pancreatitis. Bicarbonate estimation after Secretin administration. (ERCP) – invasive, not routinely done. • Indirek • Serum Trypsinogen • Pancreatic Enzymes in Stool eg chymotrypsin or elastase • Fecal Fat Excretion/Steatocrit
Kroniese pankreatitisDiagnose(2) • Beelding • Abdominale x-straal with pankreas kalsifikasies • CT Scan/MRI • Ultrasound (Conventional/EUS) • ERCP/MRCP • Ander • IgG4, ESR, RF, Calcium, Triglyceride levels
Kroniese pankreatitisBehandeling • No curative therapy available • Behandel die oorsaak. • Stop rook. Stop alkohol. • Abdominale pyn • Analgesia • Anti-oxidante • Vermindering van intra-pankreatiese druk en onderdrukking van pankreas uitskeiding • Non-enteriese bedekte ensiem vervanging • PPI • Endoskopiese behandeling • Chirurgie • Steatorrhoea • Verminder vet in diet (<20g/dag) • Pankreatiese ensiem vervanging (bv. Pancrelipase - CreonTM) • Suur onderdrukking met ‘n PPI (Verhoog duodenale pH for optimale lipase activiteit. • Diabetes Mellitus • Insulin therapie (NB. Risiko hoer vir hypoglukemie) • Ander • Supplemente, “fat soluble” vitamiene (A, D, E, K)
Kroniese pankreatitisKomplikasies • Pseudokiste • Bloeding • Pseudokiste • Pseudoaneurisme • Milt thrombose met varices wat bloei • Obstruksie (Gemene galbuis, duodenale) • Pankreas Fistel • Na Pseudokist • Externe (chirurgie) • Interne (Askites, pleurale effisie) • Kanker • Risk highest with hereditary pancreatitis and smoking • Pancreatic adenocarcinoma – CA19-9 • Dysmotiliteit • Gastroparese and antroduodenale dysmotiliteit • perigastric inflammation • hormonal changes associated with chronic pancreatitis (e.g. CCK) • side effect of narcotic analgesics.