Download

1 / 21
210 likes | 240 Vues
Learn about initiatives addressing health disparities among Minnesota’s Somali refugees, including barriers and successful interventions.

E N D
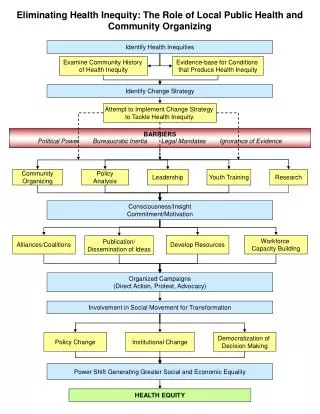
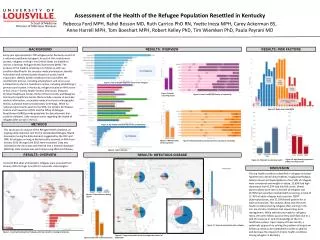
Eliminating Health Disparities within Minnesota’s Somali Refugee Population: A Community-based Approach
Nathaly Herrel, MSc1, Diana DuBois, MPH/MIA2, Saeed Fahia, PhD3, Qamar Ibrahim, MS4, Khadija Sheikh5, Faduma Abdi6, Mahmooda Khaliq, MHS7 1.Project Coordinator, Somali Health Care Initiative, Minnesota International Health Volunteers (MIHV) 2. Executive Director, Minnesota International Volunteers (MIHV) 3. Executive Director, Confederation of Somali Community in Minnesota (CSCM) 4. Executive Director, Leadership, Empowerment, and Development Group (LEAD) 5. Community Health Worker, Somali Health Care Initiative, MIHV 6. Community Health Worker, CSCM 7. Program Specialist, MIHV
Minnesota is home to over half of all Somali refugees in the US, with population estimates ranging from 10,000 to 60,000. Although Minnesota prides itself on being one of the healthiest states in the nation, there are still very large health disparities that persist within immigrant and refugee communities. • There are numerous challenges Somali refugees face including: • Accessing health care • Language and cultural barriers • lack of health insurance • unfamiliarity with the US health care system • Minnesota’s health care providers also face challenges when trying to provide culturally-appropriate quality health care for their Somali patients. To bridge the health gap that persists between the Somali community and other Minnesotans, Minnesota International Health Volunteers successfully launched the Somali Health Care Initiative (SHCI) in March 2002 in partnership with two African organizations: Confederation of Somali Community in Minnesota and the Leadership, Empowerment and Development group.
The SHCI addresses the six health disparity areas stated in Healthy People 2010 : • breast and cervical cancer • diabetes • cardiovascular disease • infant mortality • HIV/AIDS • immunizations Key activities of the SHCI include: • Training of Community Health Workers • Somali community health forums • cultural competency conferences for health providers • community-based health survey
Minnesota is home to the largest community of Somalis outside of East Africa. Community estimates range from between 10,000 and 60,000 Somali people living in Minnesota with a majority residing in the Twin Cities. The Somali community in Minnesota has had to face many challenges while adapting to life in the Twin Cities; one of these being accessing the health care system. There are many stark contrasts between the health care systems of Somalia and the US, which can make access to preventative services and treatment difficult. The agencies of the SHCI recognized the need to bridge this health disparity gap. The Somali Health Care Initiative (SHCI) is funded through the Eliminating Health Disparities Initiative of the MDH and Blue Cross Blue Shield Foundation of Minnesota.
The objectives of the SHCI are: • To increase cultural competence of providers who work with Somali patients. • To increase knowledge in the Somali community around specific health issues and to improve overall access to health care. • To increase health data about the Somali community through community-participatory research (e.g. - Somali Health Survey). • To map Somali community assets. • To build health care capacity within the Somali community by forming a cadre of Community Health Workers. • To share resources and materials with health providers, the Somali community, and relevant agencies throughout Minnesota to increase overall awareness of Somali health disparities.
The SHCI has planned and implemented activities using a participatory process: • Weekly partner meetings • Because the SHCI is a collaborative partnership between three agencies the input of all partners is critical during the decision-making process. A collaboration charter, which outlines the partnership vision, values, and roles guides the work of the partners. • Formed an advisory committee • An advisory committee of key Somali leaders and health professionals help to evaluate the appropriateness and effectiveness of SHCI health programs. The partners and advisory committee meet to discuss program activities at the outset and the conclusion of the project. • Performed Somali community asset mapping exercise • There are many resources that have been identified in the Somali community as a result of the asset mapping exercise. In addition to the formation of the advisory committee, holding meetings with Somali community organizations and identifying key Somali media and communication channels the SHCI was able to base project activities on pre-existing assets and strengths in the community and avoid a duplication of efforts.
Somali community health forums • Six health education forums were held in the Somali community on the key disease areas. The format was usually a video and/or presentation by Somali and non-Somali health providers followed by a question and answer session. This provided community members with an opportunity to interact with respected health providers as well as fostered collaboration between Somali community organizations and health providers. Forums were broadcast on Somali TV, a local cable TV program. • Conference series for health providers • Six two-hour forums geared towards health providers serving the Somali community were held to answer questions about providing quality care to the Somali community. The forums covered the major disease areas and paired Somali and non-Somali health professionals to speak on the different issues. Resources, publications and health education materials were provided to participants.
Somali women gather for breast cancer awareness activities and demonstrations. Dr. Osman and Dr. Pryce (HCMC Somali Medicine Clinic) sharing information on cardiovascular disease and diabetes at Somali Community Forum.
Somali health survey and focus group research • Health data specific to the Somali community are scarce. The SHCI designed and implemented a community-wide health survey (with funding from MDH EDHI and Blue Cross Blue Shield Foundation of Minnesota) in order to gather specific health information to better understand the health knowledge and practices of the Somali community. Further in-depth qualitative data on selected disease areas will be gathered through focus groups in 2004 - 2005. • Training of Community Health Workers • Two part-time Somali community health workers (CHWs) were hired and trained in order to bridge the gap between the Somali and health provider communities. They are responsible for translating health materials, mobilizing the community to participate in program activities, and assisting with survey questionnaire development and data collection. • Fitness classes for Somali elders • A series of fitness classes are being implemented at a community center to teach elders simple movements to stay physically fit.
Some of the successes of the SHCI: • Provider forum comments: • “I think [these forums] are the first ones I have seen specifically designed for Somali health [issues with a] combination of American health professionals and Somalis who work in healthcare here or back in Somalia.” • “[The forums were] very useful - [it] was kind of concrete in that they had some tools, books and a videotape that had been translated into Somali that were easy for me to use. Nice to hear the experience of other individuals.” • Community forum comments: • “The forum was useful because I learned a lot of information regarding mothers and babies that I did not know about. In Somalia I know that, but here in America it is different.” • “Even though I am already a mother, coming to the forum was useful because I got the opportunity to learn new things from different individuals.”
Breast and cervical cancer community forums: • Pre-post evaluation found that knowledge of breast and cervical cancer facts increased by 53% among the women who participated. • Other comments from Somali participants include: • “I learned more about this disease. Before, I thought that only those who live in America and Europe can get it. Now I know that anybody can get it regardless of where they live or what kind of food they eat.” • “It was so useful because even though I know about cancer, I still needed to know more about it and how can I protect myself from this deadly disease.” In general the community forums have been able to reach a broad audience through attendance at the forums themselves, and also via broadcast on Somali TV, which reaches 9 in 10 Somali adults.
Community mobilization and partnerships take time. • The Somali community relies on oral communication channels so it is therefore important to identify these effective channels and utilize existing networks to disseminate health information. It is essential to hold weekly partner meetings in order to keep staff informed and foster a team approach to activities. • Health competes with many other community priorities (immigration, housing, education, employment). • It is important to recognize that immigrant and refugee populations have many competing priorities that they are dealing with in addition to health. • Numerous barriers include: transportation, language, time difficulties, children. • Health education for the Somali community needs to shift to a more community-oriented paradigm. Providers have recognized that immigrant and refugee patients have difficult navigating the current health system and there are many barriers to them successfully accessing care. Therefore, the development of a more community-oriented system utilizing the expertise of CHWs will prove invaluable.
Few health education materials available geared towards the Somali community. • There is a growing need for more health education materials to be produced for the Somali community. It is not enough to simply translate the words into the Somali language; it is also essential to collaborate with community members to produce high-quality materials that are also culturally appropriate. The SHCI is filling this niche. • Health education alone is not enough to affect behavior change. • The educational materials and forums provide valuable information to the community on different health issues, however, it is important to provide an opportunity to build skills and increase opportunities for behavior change (e.g. - through fitness classes). • Health data are lacking for the Somali community. • There is a high demand for data that documents and quantifies both the health needs and assets of the Somali community. There is anecdotal evidence that there are critical health needs in the Somali community, but there is a great need for more quantitative data about knowledge levels, health practices and health system access in the Somali community. SHCI is providing some of this critical baseline information through its large scale Somali health survey.