Download
1 / 20
200 likes | 330 Vues
Case Study Emergency/Urgent Care Network Northern Minas Gerais Macroregion. Area: 122,176 Km² (São Paulo: 1,523 Km²) Population: 1,558,610 (São Paulo: 10,990,249 inhabitants) Population density: 12.6 inhab./km² (São Paulo: 7,216 inhabitants/km²). 86 cities

E N D
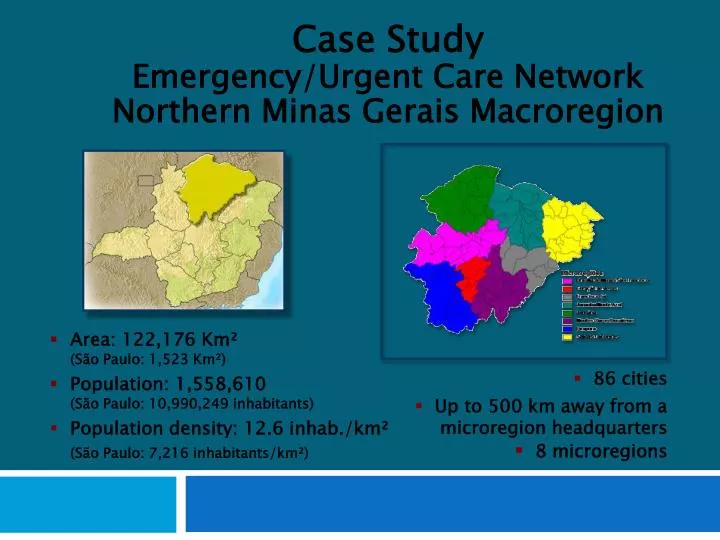
Case Study Emergency/Urgent Care Network Northern Minas Gerais Macroregion • Area: 122,176 Km² • (São Paulo: 1,523 Km²) • Population: 1,558,610 • (São Paulo: 10,990,249 inhabitants) • Population density: 12.6 inhab./km² • (São Paulo: 7,216 inhabitants/km²) • 86 cities • Up to 500 km away from a microregion headquarters • 8 microregions
Indicator: Years of Life Lost (YLL) > 1 year The leading causes of YLL among the population over 1 year of age are external causes and cardiovascular disease, which together account for more than 46% of this indicator. YLL Rate > 1 year External causes Cardiovascular disease Neoplasms Other diseases of the circulatory system Diseases of the respiratory tract Infectious/parasitic disease Diseases of the digestive tract Diabetes mellitus Others Source: SIM/DATASUS
10 Leading causes of years of life lost (YLL)in Minas Gerais, 2004-2006
Hospital-Based Emergency Care: At the Breaking Pointhttp:/www.nap.edu/catalog/11621.html
Source: Hospital-Based Emergency Care at braking point Institute of Medicine of the national academies - 2007
Correctly direct the patient… • … to the appropriate level of care • …that can provide the most effective treatment • …as fast as possible.
Economies of scale Availability of resources Quality Access
PRIMARY CARE • Call centers • Health posts (unidade basica de saúde – UBS) • Charity or small-scale hospitals (hospitais filantrópicos ede pequeno porte [HF/HPP]). Local small-scale hospitals perform a vital role within the network when access to higher-complexity services are located more than one hour away. • MEDIUM COMPLEXITY • Urgent Care Units (Unidades de Pronto Atendimento – UPA) • Microregional hospitals – these must be accessible to at least 100,000 inhabitants, some of which should provide care for more complex traumas or stabilize such patients • Emergency Mobile Care Unit (Serviço de Atendimento Móvel de Urgência – SAMU) • TERTIARY LEVEL • Macroregional hospitals with specialized services in line with preestablished parameters • Trauma Referral Hospitals – must be located within access to at least 1 million inhabitants • Hospital Referral/ CV; 400mil pop. • Rehabilitation Hospitals • SAMU • Health posts or UBS are the local care centers • Microregional/macroregional hospitals (former: more complex trauma)
THE ROAD AHEAD STEPS FOR STRUCTURING THE EMERGENCY/URGENT CARE SERVICES NETWORK • Step 1. Perform a situation analysis of the emergency/urgent care (EUC) network • Step 2. Select the model of care for the EUC network • Step 3. Develop the health districts and levels of the EUC network • Step 4. Design the EUC network • Step 5. Build the primary care component of the EUC network • Step 6. Build the secondary and tertiary care levels of EUC network • Step 7. Design network support systems • Step 8. Design network logistical systems • Step 9. Establish oversight systems for the EUC networks
Mobile Medical Unit (MMU) Basic Support Unit (BSU) Advanced Support Unit (ASU) Command Center Air TransportUnit (ATU)
Manga Monte Azul Januária Microhospital Verdelândia São João do Paraíso Rio Pardo de Minas Taiobeiras Microlevel III Trauma Hospital Brasília de Minas Microlevel III Trauma Hospital Janaúba Microlevel III Trauma Hospital São Romão Salinas Microhospital Urucuia MOC Macrolevel I Trauma and Cardiac Hospital, Santa Casa MOC Macrolevel I Trauma Hospital, Clemente Faria Francisco Sá Macrohospital MOC Macrolevel II Cardiology Hospital, Aroldo Tourinho Microhospital Coração de Jesus Fundação DilsonGodinho Pirapora Microlevel III Trauma Hospital Bocaiuva Microhospital Level III Microhospital Small-scalehospital
Hospitals/Level Basic R$ 20,000.00 Microregion R$ 100,000.00 Level III Trauma Hospital R$ 130,000.00 Level II Trauma Hospital R$ 180,000.00 Level I Trauma Hospital R$ 250,000.00 Level III Trauma and Cardiology Hospital R$ 130,000.00 Level II Trauma and Cardiology Hospital R$ 210,000.00 Level I Trauma and Cardiology Hospital R$ 320,000.00 - Level II Cardiology Hospital R$ 50,000.00 Level I Cardiology Hospital R$ 75,000.00
Results Short-Term Evaluation Process: - Progressive increase in system use: Calls to Call Center (Jan. 1,742; Aug. 7,882) Pre-hospital ambulance trips (Jan. 883; Aug: 2,904) Clinical Management: - Shorter decision-making time: critical for the outcome in the U/E - 50% drop in microregional hospital patients in green and blue risk categories: integration of primary care, and Manchester Protocol implemented throughout the network - Clinical reports
Recapping... • Emergency care systems should be based on a regional model • Emergency care systems should be under a single authority and their different points of service delivery should be coordinated • Patient flows between points of service delivery and logistics should be based on risk classification • Results of the system must be monitored • System planning and preparations are required to address sudden increases in its use • Oversight is needed to enforce rules (outsourcing) and monitor results • A new financing model is necessary, based on the adjustment of goals (replacing the fee-for-service model)
Recapping... Thank you! Antônio Jorge de Souza Marques