
Introduction
Case Report: Pregnancy outcome of a patient with jejunostomy following transhiatal oesophagectomy for functional dysphagia. Dr.S.Dexter.,Dr.D.N.Madhavan., Ms.J. Wheeler., Miss.A.Shreiner Darent Valley Hospital. Dartford., U.K. OPTIONAL LOGO HERE. OPTIONAL LOGO HERE. OPTIONAL LOGO HERE.

Introduction
E N D
Presentation Transcript
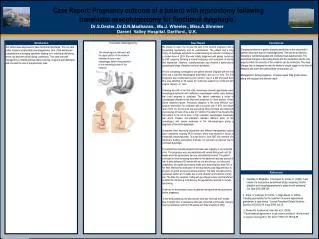
Case Report: Pregnancy outcome of a patient with jejunostomy following transhiatal oesophagectomy for functional dysphagia. Dr.S.Dexter.,Dr.D.N.Madhavan., Ms.J. Wheeler., Miss.A.Shreiner Darent Valley Hospital. Dartford., U.K.. OPTIONALLOGO HERE OPTIONALLOGO HERE OPTIONALLOGO HERE Case Report Introduction Transhiatal oesophagectomy Conclusions … We present a case of a 34 year old lady in her second pregnancy with a pre-existing jejunostomy and its complications. The patient had a long history of dysphagia symptoms to solids following an episode of choking on a chicken bone in 2003. She was initially diagnosed with globus hystericus by ENT surgeons following a normal endoscopy and symptoms of anxiety and depression. However, videofluoroscopy had showed a dysfunctional oesophageal stage of swallow and poor peristalsis. Prior to completing investigations the patient became pregnant with her first child and a planned oesophageal manometry was put on hold. The first pregnancy was complicated by poor nutrition, due to a diet of pureed food. She was admitted at 29 weeks for nutritional support but continued with vaginal delivery at term. Following the birth of her first child, manometry showed hypertensive lower oesophageal sphincter with ineffective oesophageal motility, early features that could progress to achalasia. The patient underwent a series of oesophageal dilatations that improved symptoms for short periods of time before treatment failure. Pneumatic dilatation is the most effective non-surgical intervention for achalasia with a success rate of 65% and failure rate of 30% (2). At this point she was eating 200g chocolate and drinking 6 ensures plus 20 cups of tea a day for nutrition.The patient then became the first patient in the UK to have a high resolution oesophageal manometry test which showed inco-ordination between different parts of the oesophagus with severe weakness at the mid-oesophagus giving a diagnosis of functional dysphagia. Symptoms were becoming unbearable and different management options were considered including PEG insertion, which was declined in favour of transhiatal oesophagectomy. This was done in June 2007 with insertion of a temporary feeding jejunostomy that was not removed as planned due to continued dysphagia. The patient then became pregnant and was seen regularly in our antenatal clinic. The pregnancy was uncomplicated with normal fetal growth until 24 weeks when the jejunostomy became intermittently blocked. The patient continued to have increasing discomfort in the abdomen and was warned of risk of early delivery.At 30 weeks with an oral diet of soup, ice lollies and milkshakes; the nightly jejunostomy feeds were delivering less than 50% of her feed. Mechanical obstruction of the jejunostomy was diagnosed due to pressure of gravid uterus and altered anatomy. The baby was delivered by caesarean section at 31 weeks due to port retraction and infection at entry site. The baby boy weighed 1.64kg with good Apgar scores and transferred to SCBU for monitoring. Post delivery the jejunostomy returned to normal functioning. There are no documented cases of patients having preformed jejunostomy before pregnancy. In her third pregnancy, the jejunostomy tube was removed at 27 weeks. Due to weight loss, a nasojejunal tube was reinserted at 29 weeks. Delivery was by Caesarean section at 36 weeks with baby weighing 2.35kg Our patient was diagnosed to have functional dysphagia. This is a rare entity treated by transhiatal oesophagectomy. One of the well known complications is dumping syndrome leading on to nutritional deficiency, which can become critical during pregnancy. This case was well managed by a multidisciplinary team involving surgeons and dieticians, and involved the use of a jejunostomy tube …. … The oesophagus is removed, and the upper portion of the stomach stretched to form a neo-oesophagus before being rejoined to the remaining portion of the stomach Dumping syndrome or gastric dumping syndrome is also observed in patients who have had an oesophagectomy. This can be avoided by following a nutritionist-guided and monitored well-balanced diet. The prescribed changes in the eating habits and the medication are the only ways by which the severity of the condition can be minimized. The meal change over is designed to omit the intake of simple sugars in the form of desserts and lower the carbohydrate consumption.(3) Management during pregnancy includes regular fetal growth scans, along with surgical and dietician input. References • Csendes, A; Braghetto, I; Henriquez A, Cortes, C; (1989). “Late results of a prospective randomised study comparing forceful dilatation and oesophagomyotomy in patients with achalasia.” Gut. Mar;30(3):299-304 • 2. Saha, S; Loranger, D; Pricolo, V; Degli-Espoti, S; (2009). “Feeding jejunostomy for the treatment of severe hyperemesisgravidarum: a case series.” Journal ParenteralEnteral Nutrition. Sep-Oct;33(5):529-34. Epub 2009 Jun 25. 3. Davies AR, Forshaw MJ, Khan AA, et al. (2008). "Transhiataesophagectomy in a high volume institution". World journal of surgical oncology6 (1): 88. doi:10.1186/1477-7819-6-88.





