Download
1 / 18
180 likes | 401 Vues
High mortality in Carnot city Central African Republic January-July 2012 ESCAIDE, 6 November 2013. Nelly Fournet, EPIET cohort 2011. Economical and geographical background. CAR: 4 millions inhabitants 80% of population < 2 $ / day 45% of adults are illiterate

E N D
High mortality in Carnot city Central African RepublicJanuary-July 2012ESCAIDE, 6 November 2013 Nelly Fournet, EPIET cohort 2011
Economical and geographical background • CAR: 4 millions inhabitants • 80% of population < 2 $ / day • 45% of adults are illiterate • Political instability / Isolated • Life of expectancy: 48 years
Carnot city • 61 790 inhabitants • Agriculture replaced progressively by diamond mining • 2009 : diamond mining restricted → crisis → MSF opened a programme for acute malnutrition in children • 2010 : MSF opened an HIV programme
Health situation in Carnot city • January-July 2011 : retrospective mortality survey • Crude Death Rate 3x higher than emergency threshold*: • CDR = 3.7/10,000/day (CI95% 3.0 – 4.6) • 0-5 DR = 7.0/10,000/day (CI95% 5.3 – 9.,3) → MSF actions: → Primary health care → Paediatric ward → Measles mass vaccination campaign → Mortality surveillance system *CDR = 1 death / 10,000 inhabitants / day 0-5 DR = 2 deaths / 10,000 children <5 y / day
Objectives Main objective: • Estimate the crude death rate (CDR) and the specific death rate among children <5y (0-5 DR) in Carnot city between January and July 2012 Secondary objective: • Estimate the main causes of deaths → In order to re-adjust MSF interventions
Study design • Cross-sectional retrospective survey • Recall period: January 2012 – July 2012 • Information collected: • Number of persons in the household at the date of the survey • Number of deaths / births / who joined / left the household + dates • Cause of death (simplified verbal autopsy) • Study population: • Population: all persons living more than 1 month in Carnot • Household: all persons sharing the same meal and under the responsibility of the same person
Methods • Two-stage cluster sampling • Stage one: selection of the neighbourhoods (clusters) proportional to population size • Stage two: within each cluster, selection of the households with the EPI method • Sample size: • Sample size: 3,717 persons = 710 households • 30 clusters selected: 24 households per cluster • Survival analysis: • CDR and 0-5 DR estimations and CI95% • Trends over the time
Description of the population 46% 21%
Death Rates 2011: • CDR = 3.7/10,000/day (CI95% 3.0 – 4.6) • Emergency threshold: CDR = 1/10,000/day • 0-5 DR = 7.0/10,000/day (CI95% 5.3 – 9.,3) • Emergency threshold: 0-5 DR = 2/10,000/day
Trends over the recall period Specific death rate among children <5 years from January to July 2012, Carnot city, CAR
Main causes of deaths • Children <5 years • 35% malaria • 10% neonatal deaths (without associated causes) • 7% diarrhoea • Adults >15 years • 30% HIV • 13% malaria • 10% accident (poisoning, trauma, bite…)
Conclusion • Limitations: • Recall bias • Cause of deaths reported by verbal autopsy • Results specific to Carnot City, not generalize to CAR • Crude death rate and the specific death rate among children <5y decreased half compared to 2011 • Above emergency threshold • Main cause of death: HIV among adults and malaria among children
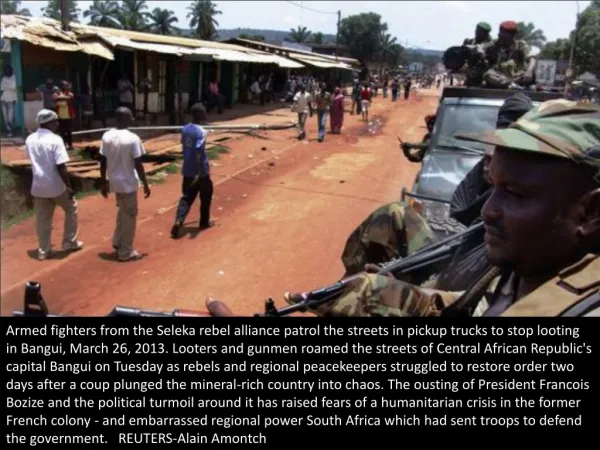
Recommendations -> Strengthen collaboration with health local authorities -> Improve access and coverage of health care centres -> Improve paediatric and neonatal health care -> Improve malaria and HIV diagnosis, treatment and prevention • March 2013 : rebellion in Bangui (capital) → Overthrow of the government → Priority: care of injured persons
Acknowledgement • Carnot city population • All Interviewers from CAR • MSF team in Carnot City • Sandra Cohuet, Epicentre, Paris • KlaudiaPorten, Epicentre, Paris • Susan Hahné, RIVM, the Netherlands
Definition of the main causes of deaths • Duration of the illness • Death linked with the pregnancy / the delivery • Neonatal death (<28 days) • Diarrhoea • Coughing / Respiratory troubles • Neurologic troubles • Malaria • Isolated fever • Measles • Trauma, injury • Pain in the mouth / difficulty to eat • Cutaneous problems / permanent scratching • Major loss of weight • Other
Case definition of HIV and TB* HIV • Duration of the illness > 2 months before death • Associated with: • diarrhoea >1 month • or difficulty to eat • or cutaneous problems • or major loss of weight • Without associated TB diagnosis TB • Duration of the illness > 2 months before death • Associated with coughing > 1 month and loss of weigh *Tassie JM, Savignoni Alexia et al. Retrospective mortality survey in Rusinga Island, Suba district, Nyanza province, Kenya. Avril 2002. Rapport final In. Paris: Epicentre; 2002.