Download

1 / 64
640 likes | 782 Vues
Systemic Therapy of Pancreatic Cancer Mark M. Zalupski, M.D. University of Michigan Providence GI Symposium November 2, 2013. Combination Chemotherapy in Advanced Disease – Current Options Investigational Approaches - Recent Disappointments, Future Promise

E N D
Systemic Therapy of Pancreatic Cancer Mark M. Zalupski, M.D.University of MichiganProvidence GI SymposiumNovember 2, 2013
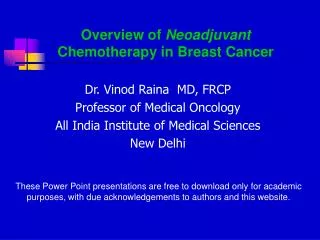
Combination Chemotherapy in Advanced Disease – Current Options Investigational Approaches - Recent Disappointments, Future Promise Systemic Therapy in Localized Pancreatic Cancer - Adjuvant Therapy and Neoadjuvant Approaches
Improvements in Survival and Clinical Benefit with Gemcitabine as First-Line Therapy for Patients with Advanced Pancreas Cancer - A Randomized Trial 126 Patients with Advanced Pancreatic Cancer Gemcitabine 1.0 g/m2 wkly x 7, rest then wkly x3 vs. 5-Fluorouracil 600 mg/m2 wkly Primary Endpoint – Clinical Benefit Response Composite of Pain (analgesic use and intensity) Karnofsky PS, Weight Required Sustained Improvement (>4 Wks) Secondary Endpoints – Response Rate, PFS, OS JCO 15:2403, 1997
Clinical Benefit Response with Gemcitabine Clin BenOS1YRPFSRR Gem 24% 5.6 18% 2.2 5% p=.002 p=.002 p=.0002 5-FU 5% 4.4 2% 1 0% Conclusion – Meaningful Clinical Activity & Low Toxicity JCO 15:2403, 1997
Phase III Gemcitabine +/- Erlotinib n=569Med Surv@ 1 Yr Gemcitabine 5.9 mos 17% p=0.023 Gem + erlotinib 6.2 mos 23% Survival Hazard ratio 0.82 p = .038 PFS Hazard ration 0.77 p = .004 J ClinOncol 25:1960, 2007
FOLFIRINOX vs Gemcitabine Metastatic Pancreatic Cancer – Survival N Engl J Med 2011;364:1817-25
FOLFORINOX Bolus 5-FU 400 mg/m2 2 h Oxaliplatin 85 mg/m2 Leucovorin 400 mg/m2 Continuous 5-FU 2.400 mg/m2 Irinotecan 180 mg/m2 2 h 46 h 1 h 30 q2wks
FOLFIRINOX vs Gemcitabine - QOL J Clin Oncol 31:23-29, 2013
Multi-institutional Experience using FOLFIRINOX n=54 treated 2010-12 (UM – KCI - Moffitt) 61% men, med age 57 (34-73), PS 0-1 91% 67% head of pancreas, 48% biliary stents 91% stage IV disease (mainly liver) 15% omitted bolus 5FU / 89% primary g-csf J Clin Oncol 30, 2012 (suppl; abstr e14519)
Median # cycles – 5 • > Grade 3 toxicity in 61% (emesis 10, fatigue 9 ANC 9, diarrhea 5, neuropathy 4, anemia 4 plts 3, infection 2, febrile neutropenia 2) • 87% required dose reduction 17% hospitalization • Partial response 39%, Stable disease 29% • Median PFS 3.8 mos (0.9-13.6) and OS 7.2 mos (0.5 – 17.8) • Treatment discontinued in 35% due to toxicities J Clin Oncol 30, 2012 (suppl; abstr e14519)
IMPACT - Study Design RANDOMIZE nab-Paclitaxel 125 mg/m2(No Premedication)+Gemcitabine 1000 mg/m2Weekly, 3 of 4 Weeks Gemcitabine 1000 mg/m2Weekly, 7 of 8 Weeks (Cycle 1) thenWeekly, 3 of 4 Weeks (Cycle 2 Onward) (1:1) N = 842 Intent-To-Treat (ITT) Stage IV No prior tx PS > 70% Measureable Dz
Systemic Therapy Pancreas Cancernot just gemcitabine anymore? Single AgentDoubletsTriplets Gem + GemcitabineErlotinibFolfirinox 5FU/Cape nab-Paclitaxel GTX Irinotecan Platin GPX 5FU/Cape Folfox / Folfiri Cape /Erlotinib
Investigational Therapy Target - Insulin-like Growth Factor 1– Receptor (IGF-1R) S0727 - Phase I then Randomized Phase II study of gemcitabine and erlotinib +/- Cixutumumab (IMC-A12) Primary endpoint PFS
SWOG S0727 Results Despite strong preclinical synergy for IGF-1R and EGFR inhibition – clinical data negative Biomarkers: Plasma [IGF], IGF mRNA predictive? Philip, P. Proceedings ASCO, 2012 Abst #4019
Investigational Therapy Target – Angiogenesis / C-MET umcc 06.076–Gemcitabine, 5FU infus, Bevacizumab n=42 median PFS 5.9 mos, OS 7.4 /mos Ann Oncol 2012 Nov;23(11):2812 umcc 09.076 – Single agent XL-184 C-MET expressed in > 70% pancreas CA Disease control rate at 12 weeks ~20% umcc 11.105 – Phase I trial of XL-184 + gem DLTs @ dose level 1(ALT/AST) Accrual ongoing dose level -1
Investigational Therapy Target – Hedgehog pathway signaling / Cancer stem cell / Stroma / Desmoplasia • Developmental pathway – neural, teeth, GI tract • Expressed abnormally in 70-80% pancreas adenoca • Activation of pathway important in carcinogenesis, progression of pancreatic cancer • Hh pathway: SMO inhibitors Cyclopamine, GDC-0449, IPI-926, LDE225 UMCC 10.003 GDC-0449 + gemcitabine
SCHEMA umcc 10.003 Metastatic Pancreatic Cancer Core biopsy for stem cell assays Daily GDC-0449 Day 22, repeat core biopsy for stem cell assays CT scan to assess disease day 28 Day 29, add Gemcitabine 1g / m2 intravenous infusion weekly x 3 every 28 days CT scans to assess response at 8 week intervals
Rand. Phase II: Gem + Vismodegib/PInterim Analysis after 50% PFS Events Correlatives: [Shh], CT perfusion Catennaci, D. Proceedings ASCO, 2012 Abst # 4022
Investigational Therapy Target – Notch signaling umcc 2013.030 A Phase 1b/2 Study of OMP- 59R5 in Combination with Nab-Paclitaxel and Gemcitabine in previously untreated Stage IV Pancreatic Cancer Target – BRCA 1-2, PALB2 mutation carriers Randomized phase II (N= 50) Cisplatin / gemcitabine +/- veliparib Gemcitabine + cisplatin d3+10, q 21 Veliparib dosing day 1-12, BID, PO
Investigational Therapy Target – RAS/MEK - mTOR/ P13K/ AKT S1115 Randomized Ph II trial comparing FOLFOX to dual pathway inhibition with AZD6244 and MK2206 Target – Tumor Stromal Depletion–PEGHP20 Pancreas cancers – high level of hyaluronan Preclinical activity for PEGHP20 Degrades hyaluronan, facilitates drug delivery Reduces interstitial fluid pressure, improved effect with cytotoxics
PEGPH20 in Advanced Pancreas Cancer • Two Randomized Phase 2 Studies • umcc 13.072 study in untreated M1 pancreas • Primary endpoint is to assess progression free survival • 124 Patients • 1:1 randomization nab-Paclitaxel/Gemcitabine +/- PEGPH20 • Currently recruiting patients • SWOG1313 study in untreated M1 pancreas • Primary endpoint is overall survival • 140 patients • Treatment with mFOLFIRINOX +/- PEGPH20 • Expected to begin in second half of 2013
Pancreatic Cancer Clinical Trials and Accrual in US • In 2011, 133 trials were open for accrual >50% of trials were based on biologic insight ~40% focused on optimization of treatment • For trials actively accruing in 2011 83% of all patients with resectable disease & 26% of all patients with metastatic disease would need to be accrued to complete accrual • Actual accrual was 4.6% J ClinOncol 2013; 31:3432
Resectable Pancreas Cancer Patterns of Treatment Failure • Early Spread to Regional Nodes • Subclinical Liver Metastasis in Majority • In Resected Pts Loco-regional Failure > 85% without Adjuvant Treatment • Liver Metastasis in > 75% Patients with Improved Local Control • Poor Prognostic Factors + LN, + margins
Adjuvant Therapy in Pancreas Cancer • Chemotherapy alone: • ESPAC-1 (5FU/LV) 2 year survival: 40 vs 30% 5 year survival: 21 vs 8% NEJM 350:1200, 2004 • CONKO-1 (Gem) Median DFS: 13.4 vs 6.9 mos Estimated 5 year DFS: 16.5 vs 5.5% Overall survival: 22.1 mosvs 20.2 mos JAMA 297:267, 2007
Adjuvant Therapy in Pancreas Cancer • Chemotherapy alone - ESPAC-3 n=1,088 Gem 1 g/m2 d 1, 8, 15 q 28 d x 6 mos vs. 5FU 425 mg/m2 LV 20 mg/m2 d 1-5 q 28 d x 6 mos med surv Gem 23.6 mos HR=0.94 p=0.39 5FU/LV 23.0 mos LBA 4505 ASCO Proc 2009
Adjuvant Therapy in Pancreas Cancer • Chemoradiotherapy (CRT): • Randomized trials and retrospective analyses have been inconsistent GITSG – Small but showed survival benefit EORTC – Negative but trend toward benefit ESPAC-1 – Large negative study with CRT Multiple uncontrolled studies suggest benefit
ESPAC Adjuvant Trial Results Randomized Participants Only (n=289) Che/RT No Che/Rtp value 5 yr surv 10% 20% 0.05 NEJM 350:1200,2004
Adjuvant Chemoradiotherapy (CRT) 472 Consecutive Pancreatic Cancer Pts (1975-2005) Complete resection (R0) (T1-3, N0-1, M0) Adverse Risk (AR) +LN (RR 1.3) High grade (RR 1.2) med OS(%) mean # ptsOS mos2yr5yr # AR No adjtx 180 19.2 39 17 1.0 CRT 246 25.2 50 28 1.2 CRT + che 28 34.8 61 34 1.4 J ClinOncol 26:3511, 2008
Adjuvant Chemoradiotherapy (CRT) 616 Consecutive Pancreatic Cancer Patients (1993-2005) R0 or R1 resections Poor prognosis high grade, size > 3 cm, R1 resection OS (%) nmed surv2 Yr5 Yr Observation 345 14.4 mos 32% 15% Adj CRT 271 21.2 mos 44% 20% Younger, healthier pts offered CRT but adjusting for risk CRT RR 0.74 ( 0.62 – 0.89 p < .001) J ClinOncol 26:3503, 2008
Adjuvant Therapy in Pancreas Cancer • NCCN Recommendation: Clinical trial preferred 5FU based chemoradiation ± gem based chemotherapy Chemotherapy alone
Adjuvant Therapy in Pancreas Cancer Univ of Michigan (UMCC) recommendation: 4 cycles of gemcitabine + cisplatin or capecitabine 5 weeks of capecitabine and radiation nR1LN+med DFSmed OS UMCC 43 14% 60% 21.7 mos 46.5 mos Conko 186 19% 71% 13.4 mos 22.8 mos RTOG 138 35% 66% NA 20.1 mos Desai et al Int J Radiat Oncol Biol Phys 75:1450, 2009
RTOG 0848 - Phase III Trial Evaluating Erlotinib and CRT Resected Pancreas Cancer Stratify by LN/CA 19-9/margin (R0/R1) Randomize to Gem +/- Erlotinib x 5 cycles if no progression, Stratify by +/- Erlotinib Randomize to CRT or not Give 1 additional cycle Chemo then +/- RT with 5FU/capecitabine Accrual Goal 950
Resectable Pancreatic Cancer Surgery additional recommendations based on surgical/pathologic findings Neoadjuvant therapy re-evaluation Surgery if not progressed with additional recommendations based on surgical and pathologic findings
Rationale for preop therapy • Provides early treatment of micrometastatic disease • Delayed recovery may prevent the delivery • of postoperative adjuvant therapy • Patients with rapidly progressive disease will not be subjected to surgery • A logical strategy for the high incidence of positive margins
Potential Barriers to Neoadjuvant Therapy • Biliary decompression • Need for biopsy EUS – FNA • Patient / Surgeon
Preop vs Postop No. Patients Benefit Morbidity Med S of of (Resected) Chemo XRT Surg Neoadj 100 60 > 20 mo Adj. 60 80 < 20 mo
Neoadjuvant Gemcitabine-based Therapy in Resectable Pancreas Cancer - MDAH Experience 1 Gem 400 mg/m2 wkly x 7 + 30 Gy RT wk 1-2 or 2 Gem 750 mg/m2 + Cis 30 mg/m2 qow x 4 Gem 400 mg/m2 wkly x 4 + 30 Gy RT wk 1-2 followed by surgery in those that remain resectable Note: only 1 of 176 pts had isolated local progression 1 J Clin Oncol 26:3496, 2008 2 J Clin Oncol 26:3487, 2008
Neoadjuvant Gemcitabine-based Therapy in Resectable Pancreas Cancer - MDAH Experience Comp/ Med Surv Med Surv n Resected Resectednot Oper Gem/RT 86 86/64 34.0 mos 7.1 mos Gem-Cis 90 79/52 31.0 mos 10.1 mos Gem/RT More difficult to complete longer preop course Most failures systemic Despite more tx in second study, poorer survival
Phase II Full Dose Gemcitabine with RTPutting the “systemic” back into neoadjuvant tx Week 1 Week 2 Week 4 Week 5 Week 6 Week 7 Week 8 M T W T F S S M T W T F S S M T W T F S S M T W T F S S M T W T F S S M T W T F S S M T W T F S S XRT XRT XRT G G G G G G G G Gemcitabine: 1000 mg/m2 30 min IV infusion XRT 36 Gy in 15 fractions
Phase II Full Dose Gemcitabine with RT n=41 8 (19.5%) ≥ grade 3 non-heme toxicity 20 pts entered as resectable 20 explored, 17 resected Clear margins in 16/17 Uninvolved LN in 11/17 One Path CR , 3 microscopic foci only Average LOS 13.5 days No 30-day mortality Median f/u 12 mos - 10/17 alive without recurrence Ann Surg Oncol 2006, 13(2):150
“Borderline” Resectable Pancreas CA Resectable “Borderline” Unresectable 15% all cases 35% all cases ~80% resected 50/50 chance < 10% resected head/uncinate neck/body/tail body surgery first “neoadjuvant” tx palliative CRT Med surv 22 mos Med surv < 12 mos Early presentation Later diagnosis Anatomic and technical considerations determine resectability
UMCC 6-25 Phase II Trial Neoadjuvant Gemcitabine, Oxaliplatin and RT Treatment Schema SURGERY ? Week 7 Week 1 Week 2 Week 3 Week 5 Week 6 M T W T F S S M T W T F S S M T W T F S S M T W T F S S M T W T F S S M T W T F S S XRT XRT XRT G G G G G G O O O O 30 Gy in 15 fractions XRT Gemcitabine: 1 g/m2, 30 minutes G Oxaliplatin: 85 mg/m2 O