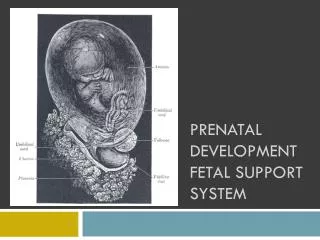
Fetal development Morphological/ physiological/ biochemical aspect and clinical correlation
Fetal development Morphological/ physiological/ biochemical aspect and clinical correlation. รองศาสตราจารย์ นายแพทย์ อติวุทธ กมุทมาศ. Morphological aspect and clinical correlation. Dating of pregnancy

Fetal development Morphological/ physiological/ biochemical aspect and clinical correlation
E N D
Presentation Transcript
Fetal developmentMorphological/ physiological/ biochemical aspect and clinical correlation รองศาสตราจารย์ นายแพทย์ อติวุทธ กมุทมาศ
Morphological aspect and clinical correlation Dating of pregnancy • Obstetricians : Menstrual age/ gestational age : LMP (first day) = 2 wk before ovulation/ fertilization , 3 wk before implantation of blastocyst • Embryologists : ovulation age/ postconception age
Clinical correlation • EDC = LMP + 7 days – 3 months • Pregnant duration = 40 wk/ 280 d/ 9 1/3 mo • 3 trimesters : 1 / 2 / 3 • Before 28 wk = abortion (USA < 20 wk) • 28 – 36 wk = preterm • 37– 42 wk = term • > 42 wk = postterm
The ovum, zygote, blastocyst • Ovulation • Fertilization of the ovum • Formation of free blastocyst • Implantation of the blastocyst
Clinical correlation • Time to test for pregnancy : serum hCG = 3 wk (gestational age) (not for UPT) • Implantation bleeding (Hartman’s sign) : 3 wk GA • Wrong date by implantation bleeding • Not include in threatened abortion
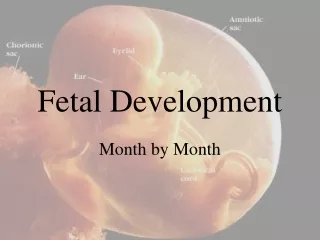
The embryo • At the beginning of the 3rd wk after ovulation (3 wk OA/ 5 wk GA) • Embryonic disc is well defined • Body stalk is differentiated • The chorionic sac = 1 cm
Clinical correlation • Time for UPT positive • Begin to detect by ultrasound : vaginal probe/ abdominal probe • GA calculated by mean sac diameter • Sac 1 cm = 5 wk GA • Sac 2 cm = 6 wk GA • Sac 3 cm = 7 wk GA
The embryo (cont) • 4th wk Ovulation age (6 wk GA) • chorionic sac = 2-3 cm in diameter • embryo = 4-5 mm in length • fetal heart beat = movement • 8 wk GA • Embryo = 22-24 mm in length • Head found and quite large
Clinical correlation • GA calculated by CRL (crown rump length) • CRL (cm) + 6.5 = GA (wk) • If bleeding = threatened abortion/ blighted ovum/ dead embryo can be diagnosed by ultrasound at this time (after 6 wk GA) • GA by CRL is accurate as ± 4.7 days
The fetus • 8wk after ovulation (GA 10 wk) • 4 cm long • Major structures are formed
12 weeks fetus • CRL = 6-7 cm • Centers of ossification appear • Fingers and toes are differentiated • Nails present • Rudiments of hair appear • External genitalia begins to show
Clinical correlation • Uterus begins to be palpable (as 1/3 above pubic symphysis) • Morning sickness is improved
16 weeks fetus • CRL = 12 cm • Wt = 110 gm
Clinical correlation • Uterus 2/3 above pubic symphysis • Doing well • Quickening • Primigravida = 18-20 wk • Multiparity = 16-18 wk • Fetal heart beat detected by stethoscope • Fetal gender detected by ultrasound
20 weeks fetus • Mid point of pregnancy • Wt = 300 gm • Fetal skin has become less transparent • Lanugo hairs cover entire body • Scalp hair visible
Clinical correlation • Uterus at umbilicus • Midpoint of pregnancy : size of uterus is mostly reliable regardless of factors such as thickness of abdominal wall, experience of the examiners
24 weeks fetus • Wt = 630 gm • Skin : wrinkled • Fat : deposit • Eyebrows / eyelashes recognizable
Clinical correlation • Uterus size = 1/4 above umbilicus (24 cm by Jeminez) • If delivered = baby (newborn/ infant) attempt to breathe , but almost always dies shortly after birth
28 weeks fetus • CRL = 25 cm • Wt = 1100 gm • Skin : red, covered with vernix caseosa • Pupillary membrane has just disappeared from the eyes
Clinical correlation • Uterus size = 2/4 above umbilicus, 28 cm • Viable period • Infant born : limbs quite energetic, cries weakly, survive with expert care (NICU)
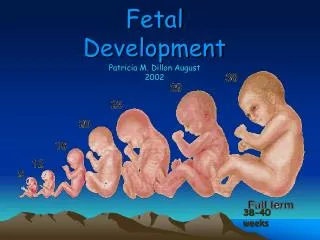
32 weeks fetus • 28 cm long • 1800 gm • Skin still red and wrinkle
36 weeks fetus • 32 cm • 2500 gm • More deposition of subcutaneous fat : wrinkle is lost
40 weeks fetus • 36 cm • 3400 gm (average) • Full term (37 - 42 weeks GA)
After 42 weeks • Postterm • Skin become wrinkle again • Amniotic fluid decreased • Placental dysfunction • Fetal compromised • Fetal death in utero/ still birth
Biochemical aspectand clinical correlation Nutrition of the fetus • First 2 months : embryo consists almost entirely of water • In later months : relatively more solids are added • Because small amount of yolk : most nutrients early obtained from mother
During the first few days after implantation : the nutrition of the blastocyst arises directly from the interstitial fluid of the endometrium and from the surrounding maternal tissue • Within the next week : intervillous spaces are formed, lacunae filled with maternal blood
Maternal diet is the source of the nutrients supplied to the fetus • If mother is fasting : glucose is released from glycogen but storage is not adequate • Cleavage of triacylglycerols (stored in adipose tissue) provide the mother with energy in the form of free fatty acid
Glucose • Facilitated diffusion • A major nutrient for growth and energy of the fetus • hPL : blocking the peripheral uptake and utilization of glucose by maternal tissue while promoting the mobilization and utilization of free fatty acid
Lactate • Transports across the placenta by facilitated diffusion • Co-transport with hydrogen ion : lactate is probably transported as lactic acid • Beware of lactic acidosis
Free fatty acid and triglycerides • Neutral fat (triglycerides) does not cross the placenta • Glycerol : cross the placenta • The apoprotein and cholesterol esters of LDL are hydrolyzed by lysosomal enzymes in trophoblasts : and give • Cholesterol for progesterone synthesis • Free amino acids (including essential amino acids) • Essential fatty acid
Amino acid • By the use of LDL • Also directly cross the placenta by diffusion
Proteins and other large molecules • Larger proteins (ie albumin) : limited transfer across the placenta • Globulin (IgG) cross the placenta in major amounts • IgM : increased amount is found only fetal infection in utero
Iron and trace elements • Active transport
Clinical correlations • Iron : active transport ; maternal iron deficiency anemia if no additional intake ; it is recommended to supplement iron in pregnancy with total 1000 mg throughout pregnancy (absorbed form) or 6-7 mg/d (absorbed form) or 30-60 mg/d (elemental form) in singleton pregnancy
IgM : indicated fetal infection • Risk of lactic acidosis : becareful in giving any drugs to pregnant women • Risk of maternal DM and fetal macrosomia : hPL (human placental lactogen), glucagon, insulinase / glucose transport is easily by facilitated diffusion