Download
1 / 31
330 likes | 554 Vues
Bennett Orthopedics & Sportsmedicine Regenerating the Youth in You!. Minimally Invasive Surgery of the Knee, Shoulder. William F Bennett MD Orthopedic Surgeon. There is a move to perform surgery through smaller incisions. Impetus- lower infection rate? less pain? quicker rehab?

E N D
Bennett Orthopedics & Sportsmedicine Regenerating the Youth in You! Minimally Invasive Surgery of the Knee, Shoulder William F Bennett MD Orthopedic Surgeon
There is a move to perform surgery through smaller incisions Impetus- lower infection rate? less pain? quicker rehab? public demand marketing product companies
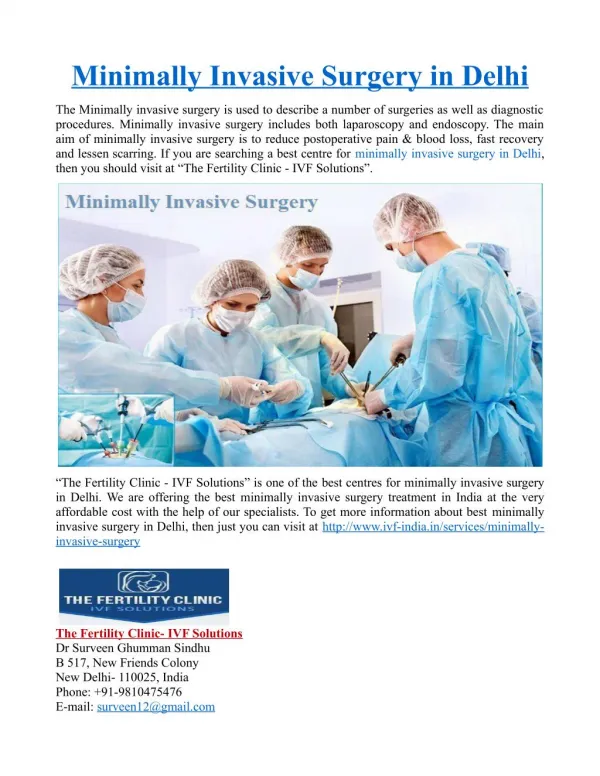
Arthroscopy vs Arthroplasty • Arthroscopy-The use of a fiber optic device and mirrors to project an image onto a television screen • Arthroplasty- replacing defective joints with implants, or other techniques to remodel the joint surface.
Arthroscopy Setup • Uses: • Knee- • cartilage • meniscus • ligaments • Shoulder- • rotator cuff • dislocation/instability • some arthritis • Hip labral tears anterior impingement
Arthroscopic Photos • Shoulder
Shoulder Arthroscopy Rotator Cuff Tears Dislocations/Subluxations Biceps subluxation SLAP Lesions Impingement Ac Joint resection Osteoarthritis
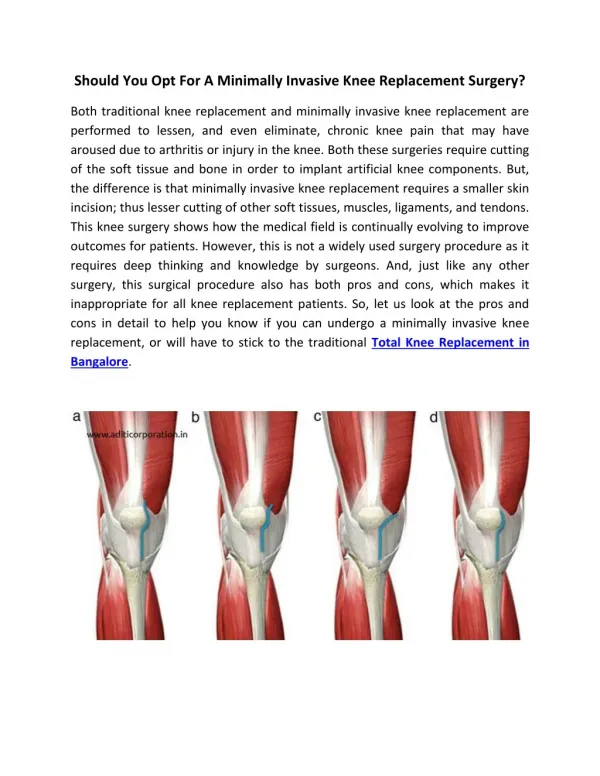
Knee Anatomy • Bones- • Femur • Tibia • Fibula • Patella
Tendons • Rectus femoris • Vastus Medialis • obliquus • Vastus lateralis • Obliquus • Patellar Ligament
Knee Arthroscopy Meniscal Repair Meniscal Resection Synovectomy Chondoplasty Ligament Reconstruction Cartilage Regeneration
Cartilage Regeneration Arthroscopic Biopsy Sent To Cambridge, Massachusetts Grown in Petri Dish Replace Deficit with open procedure Near Future- arthroscopic replacement tissue engineering
Hip Arthroscopy Limited Indications Impingement Labral Tears
However, Joint Replacement can not be done arthroscopically • However, demand has pushed us to use smaller incisions and preserve anatomy
Osteoarthritis • This knee would not be amenable to arthroscopic intervention
Mini Incision/Quad Sparing TKR • Smaller skin incision • Does not disrupt the quadriceps tendon, important for knee strength • Less time in hospital • Quicker to walk
Principles of MIS TKA Address all types of arthritic path. Approach both varus and valgus knees Provide early, exceptional analgesia Allow early hospital discharge and rapid rehabilitation The quality of the outcome not compromised by length of incision BUT NOT FOR ALL KNEES!!!!!!!!!!!!!!!!
NEW INSTRUMENTS NATURAL-LITE • MIS – Knee instruments – 4” incision
MIS TKA Intra-operative • Minimizes interruption of N/V tissue • Minimizes dissection -muscles, tendon,lig . • Avoids quadriceps disruption • Avoids disruption of the suprapatellar pouch • Eliminates patella eversion • Reduces incision length to 7 to 10 cm • Decreases blood loss • Post-operative Faster return to activities of daily living (ADL) Greater range of motion (ROM) during first six months • Leg raises and flex the knee within 6 hours • Reduced pain
Mini-Incision Hypothesis Mini TKA Standard TKA Length 20-30cm Extensive quad violation Patellar eversion Lateral release PROM PT Leg raise by POD ? Ambulate POD 1 3 - 5 days (Mean = 3.6) Blood loss Morbidity risk Lengthy rehab Length 9-14cm 1.5 - 2.0 cm Quad split Muscle relaxation Release lateral pat-fem ligament PROM PT Straight leg raise on POD 1 Ambulate POD 1 Flex to 90 by D/C < 3 days (Mean = 2.9) Blood loss Tourniquet & OR time Decreased morbidity Quicker return to ADL Reduced pain (? significant) Cosmetic appeal Exposure Rehab LOS Other Factors Reported by Dr. Luke Vaughan – Vail 2003
Quad-Sparing Hypothesis MIS TKA StandardTKA Length 8-12cm No VMO violation No patella eversion Early mobilization Leg raise on day of surgery Flex to 90 on day of surgery Ambulation day of surgery 1 - 2 days ½ blood loss Decreased morbidity Faster return to ADL Reduced pain Cosmetic appeal Length 20-30cm Extensive quad violation Patellar eversion PROM PT Leg raise by POD ? Ambulate POD 1 3 - 5 days Blood loss Morbidity risk Lengthy rehab Exposure Rehab LOS Other Factors
Small Incision • About 4 inches
Summary • Patients like the scar • Less pain • Less blood loss • Faster rehabilitation