Download
1 / 16
170 likes | 430 Vues
Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines.

E N D
Implications of Recent Clinical Trials for the National Cholesterol Education Program Adult Treatment Panel III Guidelines Scott M. Grundy; James I. Cleeman; C. Noel Bairey Merz; H. Bryan Brewer, Jr.; Luther T. Clark; Donald B. Hunninghake; Richard C. Pasternak; Sidney C. Smith, Jr.; Neil J. Stone; for the Coordinating Committee of the National Cholesterol Education Program
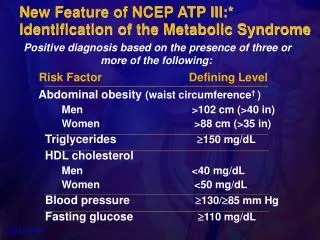
Implications of Recent Clinical Trials for the NCEP ATP III Guidelines Background • The Adult Treatment Panel (ATP III) of theNational Cholesterol Education Program issued an evidence-based set of guidelines on cholesterol management in 2001 Grundy, S. et al., Circulation 2004;110:227-39.
Implications of Recent Clinical Trials for the NCEP ATP III Guidelines Background • Since the publication of ATP III, 5 major clinical trials of statin therapy with clinical end points have been published • These trials addressed issues that were not examined in previous clinical trials of cholesterol-lowering therapy Grundy, S. et al., Circulation 2004;110:227-39.
Implications of Recent Clinical Trials for the NCEP ATP III Guidelines Objective • To review the results of these recent trials and assess their implications for cholesterol management Grundy, S. et al., Circulation 2004;110:227-39.
Log-Linear Relationship Between LDL-C Levels and Relative Risk for CHD 3.7 2.9 2.2 1.7 1.3 1.0 Relative Risk for Coronary Heart Disease (Log Scale) 40 70 100 130 160 190 LDL-Cholesterol (mg/dL) Grundy, S. et al., Circulation 2004;110:227-39.
Doses of Currently Available Statins Required to Attain an Approximate 30% to 40% Reduction of LDL-C Levels (Standard Doses) † All of these are available at doses up to 80 mg. For every doubling of the dose above the standard dose, an approximate 6% decrease in LDL-C level can be obtained. ‡ For rosuvastatin, doses available up to 40 mg; the efficacy for 5 mg is estimated by subtracting 6% from the FDA reported efficacy at 10 mg Grundy, S. et al., Circulation 2004;110:227-39.
ATP III LDL-C Goals and Cutpoints for TLC and Drug Therapy in Different Risk Categories and Proposed Modifications Based on Recent Clinical Trial Evidence Grundy, S. et al., Circulation 2004;110:227-39.
Recommendations for Modifications to Footnotethe ATP III Treatment Algorithm for LDL-C Overview of Recommendations • Therapeutic lifestyle changes (TLC) remain an essential modality in clinical management • TLC have the potential to reduce CV risk through several mechanisms beyond LDL lowering Grundy, S. et al., Circulation 2004;110:227-39.
Recommendations for Modifications to Footnotethe ATP III Treatment Algorithm for LDL-C High-Risk Persons • Recommended LDL-C goal is <100 mg/dL • An LDL-C goal of <70 mg/dL is a therapeutic option on the basis of available clinical trial evidence, especially for patients at very high risk • If LDL-C is 100 mg/dL, an LDL-lowering drug is indicated simultaneously withlifestyle changes Grundy, S. et al., Circulation 2004;110:227-39.
Recommendations for Modifications to Footnotethe ATP III Treatment Algorithm for LDL-C High-Risk Persons • Recommended LDL-C goal is <100 mg/dL • If baseline LDL-C is <100 mg/dL, institution of an LDL-lowering drug to achieve an LDL-C level <70 mg/dL is a therapeutic option on the basis of available clinical trial evidence Grundy, S. et al., Circulation 2004;110:227-39.
Recommendations for Modifications to Footnotethe ATP III Treatment Algorithm for LDL-C High-Risk Persons • Recommended LDL-C goal is <100 mg/dL • If a high-risk person has high triglycerides or low HDL-C, consideration can be given to combining a fibrate or nicotinic acid with an LDL-lowering drug • When triglycerides are 200 mg/dL, non-HDL-C is a secondary target of therapy, with a goal 30 mg/dL higher than the identified LDL-C goal Grundy, S. et al., Circulation 2004;110:227-39.
Recommendations for Modifications to Footnotethe ATP III Treatment Algorithm for LDL-C Moderately High-Risk Persons • Recommended LDL-C goal is <130 mg/dL • An LDL-C goal <100 mg/dL is a therapeutic option on the basis of available clinical trial evidence Grundy, S. et al., Circulation 2004;110:227-39.
Recommendations for Modifications to Footnotethe ATP III Treatment Algorithm for LDL-C Moderately High-Risk Persons • Recommended LDL-C goal is <100 mg/dL • When LDL-C level is 100 to 129 mg/dL, at baseline or on lifestyle therapy, initiation of an LDL-lowering drug to achieve an LDL-C level <100 mg/dL is a therapeutic option on the basis of available clinical trial evidence Grundy, S. et al., Circulation 2004;110:227-39.
Recommendations for Modifications to Footnotethe ATP III Treatment Algorithm for LDL-C High Risk/Moderately High-Risk Persons • Any person at high risk or moderately high risk who has lifestyle-related risk factors (e.g., obesity, physical inactivity, elevated triglyceride, low HDL-C, or metabolic syndrome) is a candidate for TLC to modify these risk factors regardless of LDL-C level Grundy, S. et al., Circulation 2004;110:227-39.
Recommendations for Modifications to Footnotethe ATP III Treatment Algorithm for LDL-C High Risk/Moderately High-Risk Persons • When LDL-lowering drug therapy is employed in high-risk or moderately high-risk persons, it is advised that intensity of therapy be sufficient to achieve at least a 30% to 40% reduction in LDL-C levels Grundy, S. et al., Circulation 2004;110:227-39.
Recommendations for Modifications to Footnotethe ATP III Treatment Algorithm for LDL-C Lower-Risk Persons • For people in lower-risk categories, recent clinical trials do not modify the goals and cutpoints of therapy Grundy, S. et al., Circulation 2004;110:227-39.