HIV/AIDS 2009
570 likes | 607 Vues
Learn about the etiology, pathology, epidemiology, clinical presentations, diagnosis, therapy, and health maintenance associated with HIV/AIDS. Explore the history, modes of transmission, global and U.S. statistics, clinical manifestations, diagnostic methods, and key lab values.

HIV/AIDS 2009
E N D
Presentation Transcript
HIV/AIDS 2009
Overview • Etiology • Pathology • Epidemiology • Clinical presentation • Clinical course • Diagnosis • Therapy • Health maintenance/education
Etiology • The virus • HIV causes AIDS
Etiology • RNA virus • Retrovirus, subfamily lentivirus • Cytopathic – kills cells • HIV 1 most common • HIV 2 found in West Africa – less aggressive disease, less vertical transmission • CD4 + lymphocyte is primary target but monocyte/macrohages also express CD4 and become infected
Pathology • Modes of transmission • Sexual • Vertical – mother to child, perinatal • Parenteral – injection drug users • Transfusion • Nosocomial
PathologyTransmission • Transfusion • Highest incidence during late 1970’s • Routine testing donors 1985 • Pooled coagulation factors highest risk • 8000 persons with hemophilia infected prior to 1985 • Current risk estimates 1 in 38,000 to 1 in 300,000 units of blood
PathologyCD4 + lymphocyte depletion • Direct cytopathic effects • Membrane effects, accumulation of virus, disruption of cellular RNA and protein processing • Bystander • Syncytia formation • Failure to regenerate cells • Bone marrow infection, thymus infection • Autoimmunity
PathologyOther Mechanisms • CD4 cell impairment • CD8 cell alterations • Monocyte/macrophage functional abnormalities • B cell abnormalities • Cytokines • Natural killer cells
EpidemiologyHistory • Early 1980’s • Outbreak of previously unknown illness among MSM • Virus identified in 1983 • Antibody testing of blood supply 1985
EpidemiologyGlobal • 40 million living with HIV or AIDS • 3.5 million deaths in 2001 • 4.3 million newly infected 2006 (est.) • 20 million deaths due to AIDS since beginning of epidemic
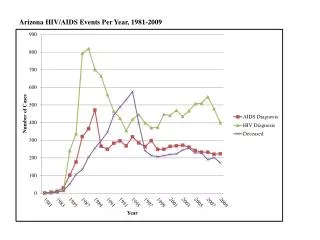
EpidemiologyUnited States • 40,000 infected each year in U.S. • One half of new infections in ages 13-24 • 17,011 deaths in 2005; 550,394 total • U.S. HIV prevalence 1.2 million • New York state has most cases • 172,377 (18%) • District of Columbia has highest rate • 128.4 per 100,000 (U.S. rate 14/100,000)
EpidemiologyUnited States • 1 million infections • 25% don’t know they are infected; in some areas 75% MSM don’t know they are infected • AIDS is reportable in all states • CDC recommends reporting of HIV; 38 states currently mandate reporting
EpidemiologyMaine • 1,256 cases since 1982 • 555 AIDS related deaths • 71 deaths in 1993 • 13 deaths in 2001 • HIV prevalence in Maine ~ 1,500 - 2,000 • One third don’t know status • MSM - 50% of cases • IDU - 20% • Heterosexual - 20%
Clinical Presentations of HIVEstablished Infection • Generalized lymphadenopathy • Unexplained thrush • New severe psoriasis, skin disorder • Unexplained weight loss • Unexplained thrombocytopenia, etc • Neurologic disease (CNS/peripheral) • Recurrent bacterial pneumonia • Chronic diarrhea
Clinical Presentations of HIVAcute HIV Syndrome • Fever • Sore throat • Swollen lymph nodes • Headache • Arthralgias/myalgias • Lethargy/malaise • Anorexia/weight loss • Nausea/vomiting/diarrhea
Clinical ManifestationsAIDS – Defining Conditions • CD4 count < 200, or < 15% • Candidiasis (not thrush or vaginal) • Invasive cervical cancer • CMV retinitis • HIV encephalopathy • Kaposi sarcoma • Mycobacterium avium, M. tuberculosis • Pneumocystis pneumonia • Progressive multifocalleucoencephaolopathy
Diagnosis • Antibody testing • ELISA/Western Blot antibody test • Rapid blood/oral test • Home HIV test kit • Viral detection • Culture • RNA PCR (viral load) • DNA PCR
Maine HIV Testing 2007 • Changes in state law • No pre-test counseling required • No written informed consent • Required • ‘A patient must be informed orally or in writing that an HIV test will be performed unless (they) decline’ • ‘Information must include an explanation of what an HIV infection involves, and the meaning of positive and negative test results’ • ‘If a test is positive, post-test counseling must be provided’
DiagnosisIndications for Testing • Behavioral risk factors • Conditions associated with infection • Recipients of blood or blood products between 1978 and 1985 • Persons with other STDs • Pregnant women • Children born to infected women or women at increased risk of infection • Occupational or non-occupational exposure
New Recommendations • HIV testing included in the routine panel of prenatal screening for all pregnant women • Repeat screen in the third trimester in areas with elevated rates of HIV among pregnant women
Home Test Kits • Collect specimen at home • Send to lab • Call for result/counseling
Key Lab Values • CD4 + Lymphocyte count • CD4 + Lymphocyte percent • HIV RNA Viral Load
Viral Load • Highest in initial infection • Key to monitoring effectiveness of antiviral therapies • Patient’s ‘set point’ determines risks/rate of progression of infection • Determines risk for maternal-fetal infection • Determines risk of occupational exposure infection
CBC Chemistries G6PD Fasting lipids Fasting glucose CXR Pap Smear PPD Urine GC/Chlamydia Serologies CMV Hepatitis A, B, C Syphilis Toxoplasma Screening Tests
Antiretroviral Therapy Sites of Action
Antiretroviral Drugs • Nucleoside Reverse Transcriptase Inhibitors (NRTIs): Zidovudine AZT (Retrovir) Didanosine ddI (Videx) Zalcitabine ddC (Hivid) Lamivudine 3TC (Epivir) Stavudine d4T (Zerit) Abacavir (Ziagen) Tenofovir (Viread) Emtricitabine (Emtriva)
Antiretrovirals cont’d • NonNucleoside RTI’s (NNRTI’s): Efavirenz (Sustiva) Neviripine (Viramune) Delavirdine (Rescriptor) • Etravirine (TMC-125)- ??? January 2008
Antiretrovirals cont’d • Protease Inhibitors (PI’s): Saquinavir (Fortovase, Invirase) Indinavir (Crixivan) Ritonavir (Norvir) Amprenavir (Agenerase) Nelfinavir (Viracept) Lopinavir/ritonavir (Kaletra) Fos-amprenavir (Lexiva) Atazanavir (Reyataz) Tipranavir (Aptivus) Darunavir (Prezista)
Antiretrovirals con’t • Fusion Inhibitor Enfuvirtide (T20, Fuzeon)
New Classes of Antiretrovirals • HIV integrase inhibitors • HIV maturation inhibitor (PA-457) • Co-receptor blockers (CCR5 antagonists)
CCR-5 Co-Receptor Antagonist • Maraviroc – August 2007 • Patients with prior experience • Only CCR5-tropic HIV-1 • Not dual/mixed CXCR4-tropic virus
Integrase Inhibitor • Raltegravir – October 2007 • Integrase strand transfer inhibitor
Treatment GuidelinesJAMA 2004;292:251-265 (July 14, 2004) Treatment for Adult HIV Infection 2004 Recommendations of the International AIDS Society-USA Panel
Treatment Guidelines • Recommendations for 4 key issues • When to start • What drugs to start with • When to change • What to change to
Special CircumstancesPostexposure Prophylaxis • Occupational • Updated U.S. public health service guidelines for the management of occupational exposures to HBV, HCV, and HIV and recommendations for postexposure prophylaxis. MMWR 2001;50(RR-11)1-67. • Nonoccupational • New guidelines: Antiretroviral Postexposure Prophylaxis After Sexual, Injection-Drug Use, or Other Nonoccupational Exposure to HIV in the United States. MMWR 2005;54(RR-02)1-20.
Concept of HIV PEP • Prevention of initial local infection and propagation of virus with antiretrovirals • Data from animal studies indicate that infection can be prevented if antiretrovirals given within 72 hours of exposure • Data from perinatal studies show efficacy even if only infant treated after birth
Nonoccupational HIV PEPIssues to Consider • Risk of transmission • Medication adverse events • Medication non-compliance • Loss to follow up • Cost • Possible increase in high risk behaviors • Possible medication resistance
Baseline and Follow-Up Testing Baseline HIV, pregnancy test, GC, Chlamydia, CBC, LFTs, chemistries Follow-up 4 weeks HIV test 3 months HIV test, Hep B and C 6 months HIV, Hep B and C 12 months HIV Need to monitor CBC, LFTs, chemistries if on PEP
Recommended Medications • NNRTI – based • Efavirenz PLUS • Lamivudine or emtricitabine PLUS • Zidovudine or tenofovir • Protease inhibitor – based • Lopinavir/ritonavir PLUS • Lamivudine or emtricitabine PLUS • Zidovudine
Special CircumstancesPregnancy • Antiretroviral medications for the health of the mother and to prevent perinatal transmission • ACTG 076 Trial – AZT for mother and infant • Recommendations based on treatment status of mother prior to pregnancy – continue meds if on, try to include AZT if possible • HIV Antiretroviral Pregnancy Registry www.apregistry.com
Immune Reconstitution Inflammatory Syndrome • Atypical inflammatory reactions that occur after initiation of effective antiretroviral therapy due to immune recognition of opportunistic infection antigens • Usually occur few weeks to several months after initiation of therapy • Usually self-limited, but manifestations may be severe (Medicine 2002;81:213-227)
Monitoring Antiviral Therapy • Adherence • CD4 and Viral Load • Baseline • 3-4 wks after start therapy • Every 4-8 weeks until undetectable • Every 3 months after stabilization • Drug Resistance Testing • Treatment failure • Before treatment initiation
What Is ‘Non-Adherence’ • Failure to take medications • Taking meds in unprescribed doses • Missing doses frequently • Taking meds off prescribed schedule • Failure to match med/dose with food as directed • Selectively eliminating 1 of meds from regimen • Sharing/selling meds • Hoarding meds for future use
HIV Resistance to Drugs • Viral conditions that lead to development of resistance: • High replication rate • High mutation rate • Selective pressure of drugs favors mutant strains over wild type; increasingly resistant strains over time