Download
1 / 30
300 likes | 330 Vues
This clinical audit assessed the compliance and effectiveness of new guidelines for red blood cell (RBC) transfusion in premature infants. It analyzed data from premature infants born between Sep 1998 and Aug 2001, comparing transfusion patterns before and after the implementation of new guidelines in 2001, and evaluated the impact on transfusion rates and phlebotomy blood loss. Results showed a significant reduction in RBC transfusions and phlebotomy blood loss after the implementation of the new guidelines.

E N D
Audit of RBC Transfusion in Premature Infants 2001 Dr Ho Hing Tung (Paediatrics) Dr Sherman Lee (Clinical Audit) Dr Raymond Chu (Haematology) Pamela Youde Nethersole Eastern Hospital
Objectives • To assess the compliance of RBC transfusion with new guidelines 2001 • To assess the effectiveness of new guidelines in reducing the number of RBC transfusions in premature infants
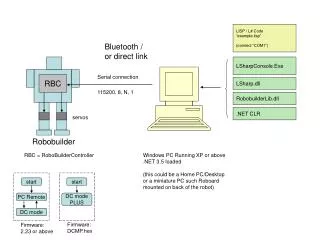
Transfusion Guidelines • Beforehand, RBC transfusion according to “Handbook of Blood Transfusion for doctors & nurses PYNEH 1998 2nd Ed.” • New RBC transfusion guideline was implemented from Jan 2001
Method • Inclusion criteria: • Inborn baby with birth weight 1500 g • Date of birth from 1 Sep 1998 to 31 Aug 2001 • Date of discharge from 1 Sep 1998 to 30 Oct 2001 • Exclusion criteria: • Babies not born in PYNEH • All perinatal & neonatal deaths before discharge • Infants required transfer out of hospital
Method • Data collection – Retrospective • All neonatal RBC transfusion episodes were retrieved from blood bank • Selection of cases according to inclusion & exclusion criteria • Trace all old records • Subgroup • BW < 1000 g • BW 1001 – 1500 g • Data collection as listed
Demographic Name ID Sex Gestation Birth weight DOB DODay 14 DODischarge Length of stay Age attain 2.2 kg Clinical First Hct % at birth Ventilation Days O2 Days BPD (36 wks PCA) IVH ( G 3) ROP ( G 3) Total no./vol. Transfusion at 2 weeks & > 2 weeks to discharge No. of donor exposure Data Collection
Compliance Indication for transfusion Compliance Old guideline New guideline Data Collection
Data Analysis • Using SPSS 9.0 • Chi-square tests for discrete variables • Student’s t tests for group means • Linear regression for prediction estimation of transfusion • Differences considered significant at a p value of < 0.05
Results • No. of premature infants included TotalTransfused% • Before • Sep 1998 – Dec 2000 45 28 62.2 • After • Jan 2001 – Aug 2001 25 8 32.0
Comparison of Transfusion Pattern Before & After New Guideline 2001
Non-compliance • Old guideline - 4 episodes • Pre-MRCP 1 • Post-MRCP 1 • FHKAM 2 • 2nd Round 3 • New guideline - 1 episode • FHKAM 1 • 2nd Round 1
Discussion • Compliance • Generally is good • Before • Old Guideline 95.3% • New Guideline 50.6% • After • Old Guideline NA • New Guideline 93.8%
Discussion • Reduction of RBC Transfusion • Before 62.2% • After 32% • Reduction of transfusion may due to • More conservative new guideline • Decreased phlebotomy blood loss • Infants were less ill • RBC transfusion rate still higher if comparing with National Institute of Child Health and Human Development (NICHD) 2001
Discussion • Reduction of Phlebotomy blood loss (ml/kg) • Before Day 14Day 15 - Discharge • 1000 41.5 41.1 • 1001-1500 22.9 18.2 • After • 1000 23.6 25.1 • 1001-1500 16.8 11.9 • Comparable to NICHD 2001
Discussion • Implementation of new guidelines can largely reduce the number of blood transfusions in premature infants • Reduction of phlebotomy loss contribute significantly to reduction in transfusion requirements • Morbidities (BPD, ROP), length of stay & age to attain weight 2.2 kg (growth) were not significantly different with the implementation of new guideline • Although our phlebotomy blood loss is comparable to NICHD, our transfusion rate is still higher • The total volume of transfusion was largely accounted by phlebotomy blood loss & ventilation days
Discussion • Speculation – with modification of guideline, limiting blood loss & use of micro-methods (POCT), non-invasive laboratory monitoring, further more conservative transfusion approach may be adopted • ? Use of Erythropoietin for preterm infants in PYNEH
Old guidelines 1998 Hct < 40% or Hb < 13 g/dl if oxygen or ventilator dependent Hct < 35% or Hb < 10 g/dl if symptomatic Hct < 27% or Hb < 8 g/dl if asymtomatic Blood loss of > 10% of blood volume New guidelines 2001 Hct 40%, severe respiratory illness Ventilator/CPAP, MAP >8 cmH2O FiO2 > 50% Severe congenital heart disease with cyanosis/heart failure Hct 35% Ventilator/CPAP, MAP 6-8 cmH2O FiO2 35-50% Hct 30% Respiratory disease requiring FiO2 25-35% / nasal cannula O2 1/8-1/4 L/min CPAP/ IPPV, MAP <6 cmH2O Sustained tachycardia (>180/min) or tachypnoea (>80/min) for 24 hours Apnoea/bradycardia 10/24 hours or 2 requiring bag mask ventilation Cessation of wt gain x 4 days Undergoing major surgery Hct 20% asymptomic Acute blood loss with shock
Discussion • Implementation of new guidelines can largely reduce the number of blood transfusions in premature infants • Reduction of phlebotomy loss contribute significantly to reduction in transfusion requirements • Morbidities (CLD, ROP), length of stay & age to attain weight 2200 g (growth) were not significantly different with the implementation of new guideline • Although our phlebotomy blood loss is comparable to NICHD, our transfusion rate is still higher • The total volume of transfusion was largely accounted by phlebotomy blood loss & ventilation days • The inverse relationship between Hct% at birth and total volume of transfusion need further analysis