Download
1 / 1
10 likes | 137 Vues
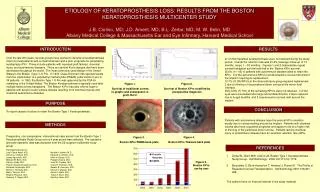
This study examines the etiology of keratoprosthesis (KPro) loss, focusing on the outcomes of the Boston Type 1 KPro, which has been instrumental for patients with corneal blindness. Over 200 years, various designs have emerged, with the Boston KPro being the most widely used in the U.S. With a retention rate of 91.6%, the results indicate that patients with autoimmune diseases face the highest failure rates due to corneal melting. This study is essential for understanding the challenges in maintaining keratoprosthesis implants in diverse patient populations.

E N D
ETIOLOGY OF KERATOPROSTHESIS LOSS: RESULTS FROM THE BOSTON KERATOPROSTHESIS MULTICENTER STUDY J.B. Ciolino, MD; J.D. Ament, MD; B.L. Zerbe, MD; M. W. Belin, MD Albany Medical College & Massachusetts Ear and Eye Infirmary, Harvard Medical School INTRODUCTON RESULTS Over the last 200 years, several groups have worked to develop a keratoprosthesis (Kpro) to treat patients with corneal blindness and a poor prognosis for penetrating keratoplasty (PK). These include patients with repeated graft failures, chemical injury, and autoimmune diseases. There are several K-pro designs that have been developed throughout the world. The most commonly used design in the United States is the Boston (Type 1) K-Pro. In 1974, Claes Dohlman first reported results from the implantation of a polymethyl methacrylate (PMMA) collar-button K-pro in 36 patients. In 1993, the Boston Type 1 K-Pro was approved by the FDA for marketing in the United States. The Boston Keratoprosthesis is typically used after multiple failed cornea transplants. The Boston K-Pro has also offered hope to patients with severe ocular surface disease resulting from chemical injuries and cicatricial autoimmune diseases. 21 of 252 implanted keratoprosthesis were not retained during the study period. Overall the retention rate was 91.6% (average follow-up of 13 months, range 1 – 53 months). Figures 1 and 2 demonstrate repeat corneal transplant survival and that of the Boston KPro survival. 25.6% (11/ 43) of patients with autoimmune disease failed to retain the KPro. 9 of the autoimmune KPro’s lost developed a cornea melt around the implant requiring its replacement. 10.7% (3/ 28) KPro’s in the chemical injury group required replacement. 2 due to thinning of the peripheral donor cornea at the donor-host interface. Only 3.8% (7/ 181) of the remaining KPro’s were not retained. 3 of the eyes were enucleated after large retinal detachments, 2 were replaced due to fungal keratitis, and 2 experienced a corneal melt around the implant. months Figure 1. Survival of traditional cornea re-graphs and subsequent re-graft, Ref 2. Figure 2. Survival of Boston KPro stratified by preoperative diagnosis PURPOSE CONCLUSION To report causes of failure to retain the Boston Type 1 Keratoprosthesis. Patients with autoimmune disease have the poorest KPro retention mostly due to cornea melting around the implant. Patients with chemical injuries also have a guarded prognosis and appear to be at a higher risk of thinning of the peripheral donor cornea. Patients lacking chemical injury or autoimmune disease have an excellent retention rate (96%). METHODS Prospective, non-comparative, interventional case series from the Boston Type 1 Keratoprosthesis Study Group over a 4 year period was collected. Pre-operative and post-operative data was analyzed from the 22-surgeon multicenter study group. Participating Surgeons: Juan-Carlos Abad, M.D. Natalie A. Afshari, M.D. Anthony J. Aldave, M.D. Eduardo C. Alfonso, M.D. James Aquavella, M.D. Keith H. Baratz, M.D. Michael W. Belin, M.D. Prabjot Channa, M.D. Kathryn Colby, M.D. John W. Cowden, M.D. Puwat Charukamnoetkanok, M.D. Claes H. Dohlman, M.D. Elizabeth Hofmeister, M.D. Sadeer B. Hannush, M.D. Ramzi K. Hemady, M.D. Marian S. Macsai, M.D. Mark J. Mannis, M.D. Samir A. Melki, M.D. Roberto Pineda II, M.D. Tueng T. Shen, M.D, Kimberly C. Sippel, M.D. Geoffrey Tabin, M.D Figure 3. Boston KPro PMMA back plate Figure 4. Boston KPro Titanium back plate REFERENCES • Zerbe BL, Belin MW, Ciolino JB. Boston Type 1 Keratoprosthesis Study Group. Ophthalmology. 2006 Oct;113(10):1779. • 2. Bersudsky V, Blum-Hareuveni T, Hehany U, Rumelt S. The Profile of Repeated Corneal Transplantation. Ophthalmology 2001:108:461-469. • The authors have no financial interest in the study material. Figure 5. Boston KPro use by year