Download
1 / 1
10 likes | 99 Vues
Competing Demands and the Quality of Diabetes Care In Primary Care Settings: A STARNet Study Michael L. Parchman, MD, MPH; Jacqueline A. Pugh, MD; Raquel Romero, MD. Results. Background and Methods.

E N D
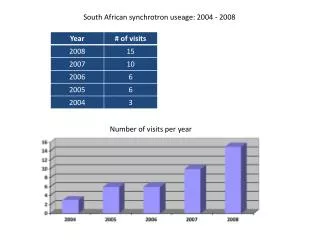
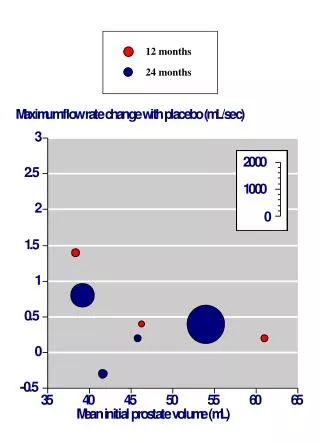
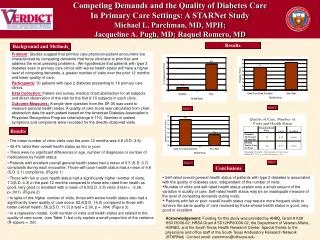
Competing Demands and the Quality of Diabetes Care In Primary Care Settings: A STARNet Study Michael L. Parchman, MD, MPH; Jacqueline A. Pugh, MD; Raquel Romero, MD Results Background and Methods • Problem:Studies suggest that primary care physician-patient encounters are characterized by competing demands that force clinicians to prioritize and address the most pressing problems. We hypothesize that patients with type 2 diabetes seen in primary care clinics with worse health status will have a higher level of competing demands, a greater number of visits over the prior 12 months and lower quality of care. • Participants:30 patients with type 2 diabetes presenting to 18 primary care clinics. • Data Collection: Patient exit survey, medical chart abstraction for all subjects and direct observation of the visit for the first 8-10 subjects in each clinic. • Outcome Measures: A single-item question from the SF-36 was used to measure general health status. A quality of care score was calculated from chart abstraction data for each patient based on the American Diabetes Association’s Physician Recognition Program criteria(range 0-110). Number of patient symptoms and complaints were recorded for the directly observed visits. Figure 2 Figure 1 Results • The mean number of clinic visits over the prior 12 months was 6.6 (S.D. 3.8). • 42.4% rated their overall health status as fair or poor. • There were no significant differences in age, number of diagnoses or number of medications by health status. • Patients with excellent overall general health status had a mean of 0.5 (S.D. 0.7) complaints during each encounter. Those with poor health status had a mean of 4.8 (S.D. 2.1) complaints. (Figure 1) • Those with fair or poor health status had a significantly higher number of visits, 7.3(S.D. 4.3) in the past 12 months compared to those who rated their health as good, very good or excellent with a mean of 6.0(S.D. 3.3) visits.(t-test = -3.36, p<.001). (Figure 2) • In spite of this higher number of visits, those with worse health status also had a significantly lower quality of care score, 52.6(S.D. 14.2) compared to those with better overall health, 56.2(S.D. 11.3).(t-test = 2.90, p = .004) (Figure 3) • In a regression model, both number of visits and health status are related to the quality of care score, (see Table 1) but only explain a small proportion of the variance (R-sqaure = .06) Table 1 Figure 3 Conclusions • Self-rated overall general health status of patients with type 2 diabetes is associated with the quality of diabetes care, independent of the number of visits. • Number of visits and self-rated health status explain only a small amount of the variation in quality of care. Self-rated health status may be an inadequate measure of the level of competing demands during visits. • Patients with fair or poor overall health status may require more frequent visits to achieve the same quality of care received by those whose health status is good, very good or excellent. Acknowledgement: Funding for this study was provided by AHRQ, Grant # K08 HS013008-02; HRSA Grant # 5D12HP00008-02; the Department of Veteran Affairs, HSR&D; and the South Texas Health Research Center. Special thanks to the physicians and office staff of the South Texas Ambulatory Research Network (STARNet) Contact email: parchman@uthscsa.edu