Download
1 / 46
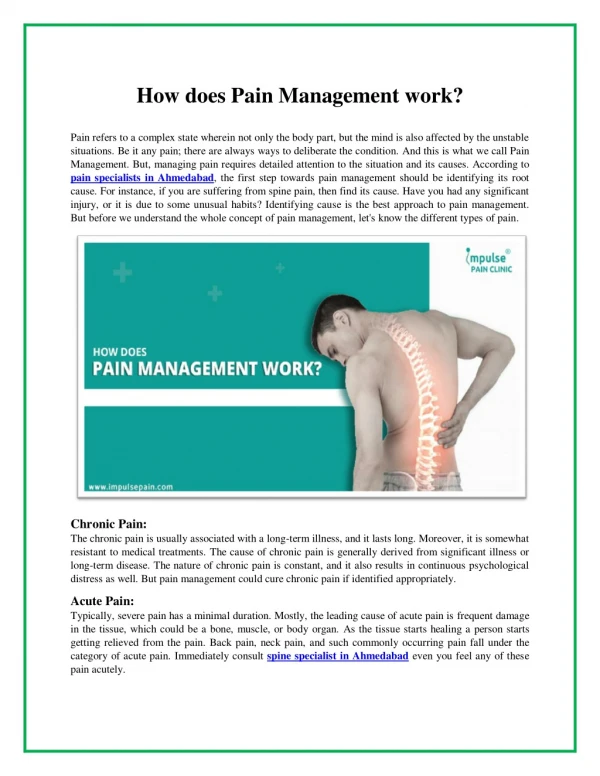
930 likes | 5.81k Vues
Management of Labor Pain. Anjani Reddy, PGY-1 1/12/09. Case Presentation. 37 y/o G1P0 @ 38wks and 1day EGA, presents complaining of ctx q5 min for 6 hours PNI: AMA: neg. quad screen, declined amnio PMH: none PSH: none PObH : none

E N D
Management of Labor Pain Anjani Reddy, PGY-1 1/12/09
Case Presentation • 37 y/o G1P0 @ 38wks and 1day EGA, presents complaining of ctx q5 min for 6 hours • PNI: AMA: neg. quad screen, declined amnio • PMH: none • PSH: none • PObH: none • PGynHx: no STIs/abnl PAPs/ovarian cysts/uterine fibroids • Meds: PNV • All: NKDA
Case Presentation • VS: stable • Exam: • SVE: 4/90/-1 • Category I tracing, ctx q 4-5min. • During initial history taking, patient was asked what her preferences were with respect to pain management. • Patient replied, “What are my options?”
Pain Pathways – 1st stage • Visceral/cramping pain during contractions • Originates in the uterus and cervix • Produced by distention of uterine/cervical mechanoreceptors and by ischemia of the uterine/cervical tissues • Signal enters spinal cord from T10-L1 • Labor pain is referred to areas of skin supplied by those nerve roots, affecting: the abdominal wall, lumbosacral region, iliac crests, gluteal areas, and thighs
Pain Pathways – 2nd stage • Somatic pain from distention of the vagina, perineum and pelvic floor • Stretching of the pelvic ligaments • S2-S4 (pudendal nerve) • More severe than first stage • Combination of • Visceral pain from contractions • Cervical stretching • Somatic pain from distention • Rectal pressure
Adverse Consequences of Labor Pain • Hyperventilation • Respiratory alkalosis could • decrease ventilatory drive between contractions • impair oxygen transfer to fetus (left shift of oxyhemoglobin dissociation curve) • Uteroplacental vasoconstriction • Neurohumoral Effects • Increase in catecholamines and decrease in blood flow to the uterus, lowering fetal oxygenation, increasing bradycardia and acidosis • Psychological Effects • Unrelieved pain may cause postpartum psychological trauma, that could result in PTSD (prevalence of postpartum PTSD found to be 5.6%)
Pain during labor and delivery • “the way pain is experienced is a reflection of the individual’s emotional, motivational, cognitive, social, and cultural circumstances” • Pain of childbirth is likely to be the most severe pain that a woman experiences during her lifetime. • Pain varies among women, and each labor of an individual may be different
Pain during labor and delivery • Pain relief was NOT the most important factor influencing satisfaction with childbirth • Study of 60 women with vaginal births found personal control was positively correlated with pt satisfaction • Study of 100 women undergoing vaginal births found that satisfaction with pain relief was associated with a feeling of being in control and having input in the decision making process.
Approaches to management of labor pain • Women should be involved in the decision-making process • Can be accomplished by educating women about pain relief techniques • Providing education BEFORE labor commences (rational decision-making is compromised at times of emotional and physical stress)
Approaches to management of labor pain • Pharmacologic – eliminate physical sensation of labor pain • Non-pharmacologic –prevent sense of suffering
Pharmacologic management of pain • Introduced in the mid-nineteenth century • Controversial-many believe that labor pain is a natural and necessary accompaniment of childbirth • Medically unusual scenario: no other circumstance in which it is considered acceptable to experience severe, pharmacologically relievable pain, while under direct medical care • Therefore, ACOG supports the concept that maternal request alone is a sufficient medical indication for labor analgesia
Pharmacologic options • Systemic analgesics • Opioids, Opioids with mixed agonist-antagonist properties, PCA, Nonopioid agents, Inhalation agents • Local injection techniques • Pudendal, Paracervical block • Neuraxial analgesia • Epidural and spinal techniques
Systemic analgesics • Opioids • Morphine • Fentanyl • Meperidine • Mixed opioid agonists-antagonists • Nalbuphine • Butorphanol • Exert effects in the maternal brain, portion of dose crosses placenta, can cause decreased fetal heart rate variability and respiratory depression in the neonate • Some argue that they produce relief by inducing somnolence rather than analgesia • Also argued that doses high enough to manage pain cannot be reached, given side effect profiles.
Meperidine (Demerol) • Dose: 25-50mg IV, 50-100mg IM • Onset: 5min IV, 40min IM • Duration: 2-3hrs • Side effect profile: respiratory depression, serotonergic crisis, seizures, and metabolite activity in the neonate for up to 2.5 days
Morphine • Dose: 2-5mg IV, 40min IM • Onset: 3-5min IV, 20-40min IM • Duration 3-4hr • Side effects: Greater respiratory depression in mother/infant than Demerol
Fentanyl • Dose: 25-50mcg IV, 100mcg IM • Onset: 1-3min IV, 7-10min IM • Duration: 1-2hrs IM • Side effects: respiratory depression • Remifentanil is in the same subclass – same onset, but metabolized quickly, thus, should not cause respiratory depression
Mixed Agonist-Antagonists • Butorphenol, Nalbuphine, Pentazocine, and buprenorphine • Dose ceiling effect – in terms of respiratory depression (can intensify analgesia without increasing respiratory depression). • Besides opioid side effects, also have psychomimetic effects • Less frequently used, mixed properties thought to diminish efficacy
Other systemic analgesics • PCA pump • Antiemetics: Hydroxyzine and promethazine • Nitrous Oxide – used in UK. Self-administered. Short acting. Inexpensive, easy to administer, safe for mother and fetus/neonate, and improved analgesia compared to opioids. • Ketamine, Benzos, and Barbituates have been used to improve sleep during early labor, or for sedative purposes. • Scopolamine – used for “twilight sleep” in early 20th century. Rarely used today.
Neuraxial Techniques • Used by more than 70% of women who give birth in hospitals with greater than 1500 deliveries per year • Spinal vs. Epidural techniques • Immediate onset vs lower side effect profile • Side effects include hypotension, fever, HA, numbness, and infection
Epidural • Continuous infusion of: • Local anesthetic (Bupivacaine or Ropivacaine) • Opioid (usually lipid soluble Fentanyl or Sufentanyl • +/-Epinephrine (works on alpha 2 receptors)
Pudendal Nerve Block • Alleviates pain arising from vaginal and perineal distention • Used as a supplement for epidural analgesia if the sacral nerves are not sufficiently anesthetized • Provide analgesia for low forceps delivery
Systemic vs. Regional analgesia • Systematic Review found: • Opioids provided limited pain relief, only slightly better than placebo • Epidural analgesia provided better pain relief than parenteral opioids • Epidural analgesia assoc with longer duration of labor, increased Pitocin augmentation, more instrumental deliveries • Effect on c-section rate varied by study
Randomized trial of Epidural vs IV Demerol analgesia for the initial treatment of labor pain • 1,330 pts • Increased rate of c-section delivery secondary to dystocia in the epidural anesthesia group (OR = 1.98, 9% vs 5%) • Epidural associated with • Increased pain relief (60% vs 22%) • Increased chorioamnionitis (23% vs 5%) • Increased Pitocin use (32% vs 23%) • Increased low forceps delivery (8% vs 1%)
Approaches to management of labor pain • Pharmacologic – eliminate physical sensation of labor pain • Non-pharmacologic –prevent sense of suffering
Non-pharmacologic approach Goal is to eliminate her sense of: • Perceived threat to body and/or psych • Helplessness, loss of control • Distress • Insufficient resources for coping with the situation • Fear of death of the mother or baby
Non-pharmacologic approach • Pain is a side effect of a normal process • Goal is NOT to make the pain disappear • Instill self-confidence, sense of mastery and well-being • So that pain is neither feared, nor focused on • Women who feel that they have successfully coped with the pain and stress of labor note that they were “able to transcend their pain and experience a sense of strength and profound psychologic and spiritual comfort during labor.”
Birth Environment • Promotes sense of comfort and privacy • Comfort aids • Places to walk, bathe, and rest • Study comparing hospital vs home births found hospital births were associated with higher pain ratings • Systematic review of randomized trials of home-like versus conventional institutional settings for birth • Increased likelihood of not using intrapartum analgesia/anesthesia (RR1.19, 95% CI 1.07-1.21) • Request same setting the next time (RR1.81, 95% CI 1.65-1.98) • Express satisfaction with intrapartum care (RR1.14, 95% CI 1.07-1.21)
Continuous Labor Support • Nonmedical care of laboring women throughout labor and delivery by a trained person • Supportive companion during labor can help with pain and anxiety • Multiple studies have shown that doulas: • Half the risk of unplanned c-sections • Half the risk of instrumental delivery • Significantly shorten labor
Water Immersion • Warm water, deep enough to cover the woman’s abdomen • Enhances relaxation, reduces labor pain • Body temperature should be monitored • Few minutes to hours in the first stage of labor • Randomized trials show: • Significant reduction in pain (via pain score or decreased narcotic use) • No increase in infection rates (even c ROM)
Intradermal Water Blocks • Incidence of low back pain in labor is 15-74% • Etiologies include: asynclitism, fetal OP position, referred uterine pain, lumbopelvic characteristics • Endorphins release thought to be responsible for pain relief • Randomized trials have found: • Significant decrease in severe LBP • Relief lasts 45 -120 minutes
Intradermal Water Block • 4 intradermal injections of .05-.1mL sterile water with a 25 gauge needle. Over each posterior superior iliac spine and two 3cm below and 1cm medial to the first sites. • Burning during injection, therefore, given during ctx.
Maternal Movement and Positioning • 76% of hospitalized laboring women do not walk around. Limited movement was secondary to: • Connections (IVs, tocometers, BP cuffs, catheters) • Pain medications • Instructed not to by medical staff
So many positions, so little time! • Knee-Chest* • Dangle • Hands and Knees* • Labor Dance* • The Lift* • The Lunge* • Rocking • Side Lying* • Squatting • Toilet Sitting • Tug of War • Walking and Swaying* • Semi-prone* • Rhythmic ritual for handling contractions • Pelvic dimensions vary with different maternal positions, ameliorating labor pain • *Certain positions are specifically helpful when back pain is the primary cause for discomfort
Movement during the 1st stage • 16 controlled trials: • Less pain while standing/sitting, compared to supine • Compared to lying on one’s side, less pain while sitting, until 6cm, then less pain while lying on one’s side • Vertical and side lying positions were accompanied by more progress than the supine position • High satisfaction associated with the option of walking
Movement during 2nd stage • Supine position found to be more painful than other positions • Kneeling position preferred to sitting position
Touch and Massage • Touch communicates caring, concern, reassurance, and love • Massage enhances relaxation and reduces pain • Have been found to decrease pain, anxiety and blood pressure • Shown to improve mood, and sense of support • NO harmful effects!
Application of Heat and Cold • Personal choice • Place one or two layers of cloth to protect against skin damage and intact sensation is a prerequisite • Heat • Applied to back, lower abdomen, groin, perineum • Relieves pain, chills, stiffness, muscle spasm, and increases extensibility of connective tissue • Cold • Applied to back, chest, face • Relieves pain, muscle spasm, inflammation and edema
Childbirth Education • Reading, classes, office visits • Information on the process of labor and birth, typical pain experience, and options for pain management should be provided for pregnant women and partners/supports. • Provision of education PRIOR to labor!!
Relaxation and Breathing • Rhythmic breathing patterns that promote relaxation, and distract women from labor pain • Enhance sense of control • Survey of women who gave birth in the US in 2005: • 49% used breathing techniques • 77% found these helpful • 22% did not • Study of British women using relaxation techniques: 88% found techniques helpful
Music and Audioanalgesia • Few studies, with small sample sizes and inadequate controls • Cochrane review on the effect of music on acute pain • Small reduction in pain intensity levels and opioid requirements
Aromatherapy • Use of concentrated oils distilled from plants • Use is increasing • Some sources note that they are potent as pharmacological drugs and should be used with caution • One uncontrolled prospective study 8058 women Lavender, rose or frankincense used under supervision of midwives Used to decrease fear, anxiety, pain, nausea and vomiting Half of women found it helpful 1% reported nausea/headache as side effect
Acupuncture/Acupressure • Acupressure is a simpler alternative to acupuncture, pressure applied with fingers or small beads at acupuncture points • Both have shown to lead to lower use of pharmacologic pain relief • Acupuncture has been shown to increase relaxation in laboring patients
Hypnosis • “a state of deep physical relaxation with an alert mind, in this state, the subconscious mind can be more readily accessed” • Self hypnosis: “glove anesthesia”, “time distortion”, “imaginative transformation” • Significant reduction in analgesic use • Contraindicated in women with history of psychosis
Transcutaneous Electrical Nerve Stimulation • Low voltage impulses to the skin via surface electrodes • Rentals available w/o rx • Paravertebrally at T10-L1 and S2-4 • Woman controls intensity and sensation patterns • Increases endorphins • Randomized trials showed • Decreased and later introduction of pain meds • Reduction of pain scores was shown in some studies
Case Presentation Continued… • 6PM: Patient admitted. • Options discussed. Patient expressed interest in systemic analgesics • Preference presented to OB staff • OB staff felt epidural analgesia would improve patient’s pain control and provide long-term pain relief • This option was presented to the patient again, and patient agreed with epidural analgesia • 7:30PM: Epidural placed • 12:30PM: Unplanned C/S performed 2/2 “non-reassuring heart tones”
Resources • Ramin, S. Randomized Trial of Epidural vs. IV analgesia during labor. ObstetGynecol 1996 Nov; 86(5): 783 • Lowe, NK. The nature of labor pain. Am J ObstetGynecol 2002; 186:So16 • Goetzl, LM. ACOG Practice Bulletin. Clinical Management Guidelines for OB-Gyns Number 3, July 2oo2. Obstetric analgesia and anesthesia. ObstetGynecol 2002; 100:177. • Simkin, P. Comfort in Labor. Childbirth Connection. • www.utdol.com • www.pregnancytobaby.com/.../medical-treatments/ • homepages.ed.ac.uk/asb/SHOA2/chpt2.htm • Creedy, DK. Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth 2000; 27:104 • Bricker, L. Parenteralopioids for labor pain relief: A systematic review. Am J ObstetGynecol 2002; 186:S094 • Bucklin, BA. Obstetric anesthesia workforce survey: twenty-year update. Anesthesiology 2005; 103:645 • Hodnett, ED. Home-like vs conventional institutional settings for virth. Cochrane Database Syst Rev 2005; CD000012 • Ragnar, I. Comparison of the maternal experience and duration of labour in two upright delivery positions – a randomized controlled tril. BJOG. 2006; 113:165 • Simkin, P. Nonpharmacologic relief of pain during labor: Systematic reviews of five methods. Am J ObstetGynecol 2002; 186:S131 • DeClercq, ER. Listening to mothers II: Report of the Second National Survey of Women’s Childbearing Experiences. Childbirth Connection, New York 2006. • Mantle, F. The role of hypnosis in pregnancy and childbirth. Ch 10- Complementary Therapies for Pregnancy and Childbirth. 2nd Edition. BalliereTindall, New York 2000. • Cepeda MS. Music for pain relief. Chochrane Database Syst Rev 2006; CD004843 • http://birthingnaturally.net/