Download
1 / 27
270 likes | 292 Vues
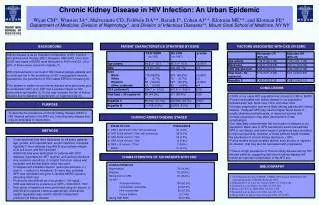
Learn about Nephropathia epidemica caused by Puumala hantavirus, its clinical course, diagnosis, and renal involvement. Discover risk factors, prognosis, and long-term consequences.

E N D
Kidney disease in Puumala hantavirus infection Prof. Jukka Mustonen University of Tampere, Tampere University Hospital, Finland
HFRS; hemorrhagic fever with renal syndrome Hantaan-, Seoul-, Dobrava-, Saaremaa- ja Puumala-virus HCPS; hantavirus cardiopulmonary syndrome Sin Nombre-, New York-, Andes-virus etc. Hantavirus infections
Nephropathia epidemica caused by Puumala hantavirus (PUUV) • Puumala hantavirus • Inhaled aerolos of bank vole excreta and secreta (urine, feces, saliva) via respiratory tract • PUUV remains infective for several weeks • Thousands of cases annually in Finland, 1000 serological diagnoses • Sweden,Norway,DenmarkIceland ? Myodes glareolus
Nephropathia epidemica (NE) • Incubation period 2 – 4 weeks • Typical patient is 40 year-old male (70 %), anamnestic contact to bank vole • Risk factors for infection: forestry, farming, camping, summer cottages, crises (Balkan), smoking • Rare and mild in children • Totally asymptomatic – Fatal course • Case-fatality rate 0.1–0.4 %
Clinicalcourse of NE (Vapalahti et al, Lancet Infect Dis 2003) 5
Increased capillary permeability • Hemoconcentration, hypotension and shock, ascites, pleural effusion and pulmonary edema • Cytokines produced by various cell-types • Beeta-3 integrins regulate vascular integrity, endothelial cell permeability and platelet functions • VEGF induces vascular permeability • VE-cadherin is a component of endothelial cell adherens junctions • Complement is activated via alternative pathway • Bradykinin (BK)
Vasculopathy in hantavirus-mediated diseases Vaheri et al 2013 Nat Rev Microbiol
Immunity • Long-living immunity. PUUV-antibodies observed 50-years after acute NE (Settergren et al, Lancet 1991) • Recurrent PUUV-infection has not been described • Long-lived memory T lymphocyte responses after NE (van Epps et al. J Exp Med 2002)
Diagnosis of NE Anamnestic data aboutbankvoles Clinicalpicture: Fever, headache, abdominalpains Laboratory: proteinuria (+++), hematuria (++), elevated s-creatinine, thrombocytopenia, CRP IgM-class PUUV-antibodieseven at theacutephase Renalbiopsy is usuallynotneeded in thediagnosis of AKI in NE
NE and the kidney • Transient, sometimes massive PU • Microscopic,rarely visible hematuria • Acute kidney injury (AKI) • Electrolyte abnormalities (hyperkalemia) rarely severe • Dialysis treatment in 5% of hospital treated patients • Acute tubulointerstitial nephritis
Acute tubulointerstitial nephritis • Interstitialinfiltrates of lymfocytes, monocytes and polymorphonuclearleukocytes • Tubular LM-changes • Peritubular cytokines • Slight LM-changes in glomeruli • Podocyte EM-changes • Medullaryhemorrhagias in 25% • PUUV present in renaltissue No correlation between histological findings and the amount of proteinuria Mustonen et al. 1994, Temonen et al. 1996, Krautkrämer et al. 2011, 2013 Boehlke et al. 2014
Urinary albumin exretion correlates with maximun urinary IL-6 excretion in NE Local IL-6 production in inflammed kidneys is possible Mäkelä et al, Am J Kidney Dis 2004
Soluble urokinase-type plasminogen activator receptor (suPAR): role in the development of PU in NE Outinen et al. J Intern Med 2014
Renal ultrasound findigs (Paakkala et al. Acta Radiol 2002) • Transiently enlarged kidneys in all patients • 57% had also fluid collections: perirenal, pericardial, pleural, ascites fluid • Alterations correlate with the severity of AKI and the amount of fluid retention
MRI: enlarged kidneys and fluid collections Paakkala et al. Eur Radiol 2005
Acute kidney injury (AKI) in PUUV infection (own studies 2015-2017) • In contrast to worldwidewell-accepted KDIGO criteria, evensevere AKI hasa goodprognosis • Active smoking is associatedwithsevere AKI • Glomerularproteinuria(PU) butnottubular PU associateswiththeseverity of AKI • Combinedresult of hematuria and PU in thedipsticktestat hospitaladmissionclearlypredictstheseverity of upcoming AKI • Thrombocytopeniadoesnotassociatewith AKI
HLA-haplotype B8DR3 and the clinical picture of NE (Mäkelä et al. 2002)
Biomarkers of the severity of AKI in NE • CRP: AKI protective • Cf-DNA: AKI - No • IL-6: AKI - Yes • PTX3: AKI – Yes • IDO: AKI – Yes • suPAR: AKI – Yes • GATA-3: AKI – Yes • Outinen et al. 2010, 2011, 2012, 2013, Libraty et al. 2012
Prognosis of NE • 5 years after acute NE patients had higher blood pressure, higher glomerular filtration rate (GFR) and more proteinuria (PU) compared to controls • 10 years after acute phase there were no differences in GFR and PU • Some patients had developed hypertension • Tubular proteinuria (alpha-1—microglobulin) was more common in patients also in this phase (Remnant kidney damage?) Mäkelä et al. Kidney Int 2000, Miettinen et al. Kidney Int 2006
Long-term nephrological consequences of NE • Depressedtubularfunction • Glomerularhyperfiltration • Proteinuria • Hypertension • Membranoproliferativeglomerulonephritis, 10 casesin whomnephroticsyndromeemergedduringconvalescentphase, goodprognosis(Mustonen et al. 2001, Mäkelä et al. 2007)
Recent reviews by Tampere and Helsinki group • Vaheri A, Henttonen H, Voutilainen L, Mustonen J, Sironen T, Vapalahti O. Hantavirusinfections in Europe and theirimpact on publichealth. RevMed. Virol 23: 35-49, 2013 • Vaheri A, Strandin T, Hepojoki J, Sironen T, Henttonen H, Mäkelä S, Mustonen J. Uncoveringthemysteries of hantavirusinfections. NatureRevMicrobiol 11: 539-550, 2013 • Mustonen J, Mäkelä S, Outinen T, Laine O, Jylhävä J, Arstila P, Hurme M, Vaheri A. Thepathogenesis of nephropathiaepidemica: New knowledge and unansweredquestions. AntiviralRes 100: 589-604, 2013 • Mustonen J, Outinen T, Laine O, Pörsti I, Vaheri A, Mäkelä S. Kidneydisease in Puumala hantavirusinfection. Infect Dis (London) 49: 321-332, 2017