Download
1 / 16
160 likes | 586 Vues
The psychosocial impact of Klinefelter syndrome. A 10 year review. Background. Klinefelter syndrome (KS) 2 nd most common chromosomal disorder Prevalence 1 in 600 males (population studies) 47 XXY karyotype predominantly. Phenotype.

E N D
The psychosocial impact of Klinefelter syndrome A 10 year review
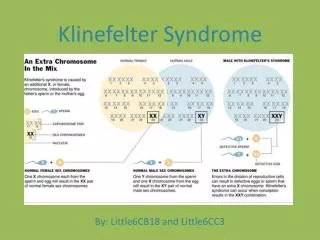
Background • Klinefelter syndrome (KS) 2nd most common chromosomal disorder • Prevalence 1 in 600 males (population studies) • 47 XXY karyotype predominantly
Phenotype • Classic phenotype of tall stature, eunuchoid body habitus, poor musculature, sparse facial hair, small testes, gynaecomastia • Significant learning impairments, predominately with language acquisition • Association with Type 2 diabetes mellitus, autoimmune disorders (eg thyroiditis/ coeliac disease), maligncies including testicular teratoma/seminoma, yolk sac tumour, male breast cancer, leukaemia
Phenotype cont • Often only present when fertility problems • Majority remain undetected (up to two thirds) - usu have decreased gonadal size, elevated gonadotrophins, decreased bone mass
Objectives • Describe psychosocial morbidity in KS • Document the effect of androgen replacement on behaviours • Underline issues confronting clinicians involved in their management • Demonstrate the need for structured program for prospective intervention
Patients and methods • Retrospective clinical case audit of pts with KS from RCH Melb 1994 – 2004 • Medical records using ICD10 coding, Dept of Endocrine database and consultants’ memories • Data collected from pt notes only • Given interest in effects of testosterone deficiency/replacement, postpubertal pts studied only
Results • 42 pts with KS were found • 32 of these pts were postpubertal • Median age 24.5yrs • 11/32 (34%) - Gynaecomastia • 3/32 (9%) – Epilepsy • 5/32 (16%) – Undescended testes • 3/32 (9%) - Malignancy
Diagnosis • 8/32 – diagnosed in childhood following chromosomal analysis as part of Ix for dev delay/behavioural disorder • 11/32 presented with pubertal delay/arrest
Hormonal replacement • 17/32 required testosterone treatment (administered via s/c pellet) • 11/32 – testosterone replete despite raised FSH/LH • 3/32 – lost to follow up, 1/32 deceased (ALL) • None had used ICSI for Mx of infertility
Psychosocial characteristics • 23/32 – documented problems with aggression/impulse control • 9/32 police involvement • Drugs/alcohol (3) • Rape/attempted rape (4) • Theft (4) (NB – 2 multiple charges)
Psychosocial cont • 6 pts – convictions, 2 incarcerated • Repetition of offences characterises the group • Poor self esteem, depression and aggression – repeated job losses/failure of permanent employment • Morbid depression with suicidal ideation a characteristic pattern
Psychosocial cont • Documented learning difficulties in 23/32 pts • None had achieved a tertiary education
Change in behaviour with testosterone • 8/17 pts on regular (24 weekly) testosterone treatment intermittently late by 1- 2 months • Exacerbation of psychosocial disorder with increased frequency of job loss and/or criminal events documented for 17 events in these 8 pts
Comparator group - Kallmann syndrome • Hypogonadotrophic hypogonadism, no known behavioural phenotype • 21 pts in same time frame • Major issue - isolated testosterone deficiency • Predominantly normal psychosocial profile • 5 - mild depression, 4/5 mild aggressive tendency, alleviated by T therapy
Discussion • Testosterone in hypogonadal males leads to amelioration of aggression rather than exacerbation • Poor executive function and aggression leads to predictable pattern of behaviour in severely affected KS pts • Vicious cycle of poor planning and impaired judgement, then failure to learn from mistakes
Discussion cont • No formal structure in place to assist men with KS either for ongoing physical surveillance or psychosocial support