Enhancing Diabetes Care in Cambodia through Peer Educator Networks
220 likes | 293 Vues
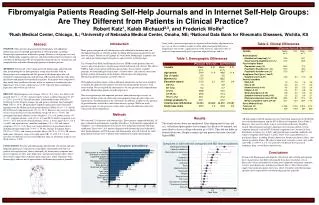
Integrating Diabetes Peer Educator networks in primary healthcare is crucial for low-income countries like Cambodia. This thesis explores the impact of such networks on early detection, cost containment, and quality of life for diabetic patients.

Enhancing Diabetes Care in Cambodia through Peer Educator Networks
E N D
Presentation Transcript
MoPoTsyo Patient Information Centre Maurits van Pelt CambodiaDiabetes self-help groups
Diabetes Peer Educator networks should be integrated in the primary health care system Our Main Message
But most Health Policy makers say “Chronic Disease interventions are not cost effective” “Chronic Diseases are a black hole, especially for secondary prevention among patients……..”
Cambodia Health Sector Donors . External assistance focus by programs budgets only 1% for Non Communicable Diseases (NCD) although they cause more than half of disease and death
We say: This lack of policies….breeds poverty! Markets move fast to grab opportunities; Markets create confusing information; Product safety concerns increase Willingness-to-Pay Biggest spender on product promotion wins Consumers do not know what would be their best choice The market’s natural response is supply side centred; All factors combined: It leaves many unmet needs… Premature disability replaces productivity
Lack of trained Doctors and Nurses; After training, they are severely underpaid; Public health system is only for acute cases; Chronic patients supplement health staff income…; A profitable patient is an ignorant one…; Question: If formal health staff has no incentive to transfer knowledge + skills to chronic patients……then who has ? Elements of the Diabetes context
We often assume that we understand the problems We set priorities for low income countries…. This can be terrifying.. Diabetics are: Rich.. ? Overweight.. ? Old.. ? Too low educated to self-manage?
Proposed thesis : “Diabetes Peer Educator Networks are a worthwhile investment for Low Income Countries in Asia like Cambodia”
Demand side organisation in NCD A Diabetes Peer Educator Network in an Operational District (a.k.a. zône de santé) led by a manager (a.k.a. DPM) in charge of community based Diabetes Peer Educators
The Diabetes Peer Educator Is a self-managing Diabetes patient who may have any profession except health service provider & • Is Literate • Is Volunteer • Was trained 6 weeks in Diabetes Peer Education • Has passed the Peer Educator exam
A) Understand how they can keep their blood glucose and blood pressure always within the safe margins: lifestyle (type of food, exercise, kg) right medication self-measuring B) Understand how they can keep this affordable; What do DM patients actually need ?
Immediate Effects: Distribute urine glucose strips for self - testing: one per adult; Detect DM earlier (70% did not know it) Increase reservoir of aware DM from 30% to 41% in Yr 1 (Yr 2 > 50%) Peer Educator Assesses: Presence of Urine glucose Fasting Blood Glucose Blood Pressure Heart rate BMI Waist circumference Feet inspection, nerve d. etc. …..reports to her/his DPM Benefit 1: Earlier Detection
Benefit 2: Transfers Knowledge + skills
Benefit 3: Lifestyle changes <12 months
Benefit 4: No stress on health services • Benefit 4: Avoiding early medicalisation728 Medical Consultations in 15 months Average 1.8 consult per patient, 160 DM did not yet meet with the Doctor
Benefit 5: Cost Containment 1 million patients: 350.000 DM + 700.000 High BP Annual drug bill remains too high if supply side controls while the demand side pays (USD 250 million). Annual drug bill can be low, if demand side controls AND pays (USD 40 million, is mostly affordable…); There will still be a role for targeted subsidies for new poor DM;
DM Patients feel better because they: Regain control over their health Spend less than before on health care Can get health information that they need Benefit 6: Quality of Life
Benefit 7: Biological outcomes
Benefit 7: Overall lower BG
Example Ang Roka OD 133.000 inhabitants Example Ang Roka OD 133.000 inhabitants
USD 6700 per year for 665 (2nd year-) diabetics USD 10 per diabetic per year at current levels A Peer A Day Keeps the Doctor Away! Peer Educator network running costs www.mopotsyo.org