Download
1 / 40
400 likes | 421 Vues
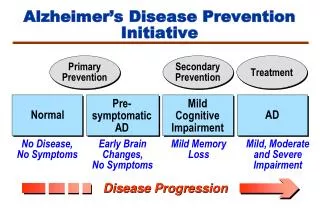
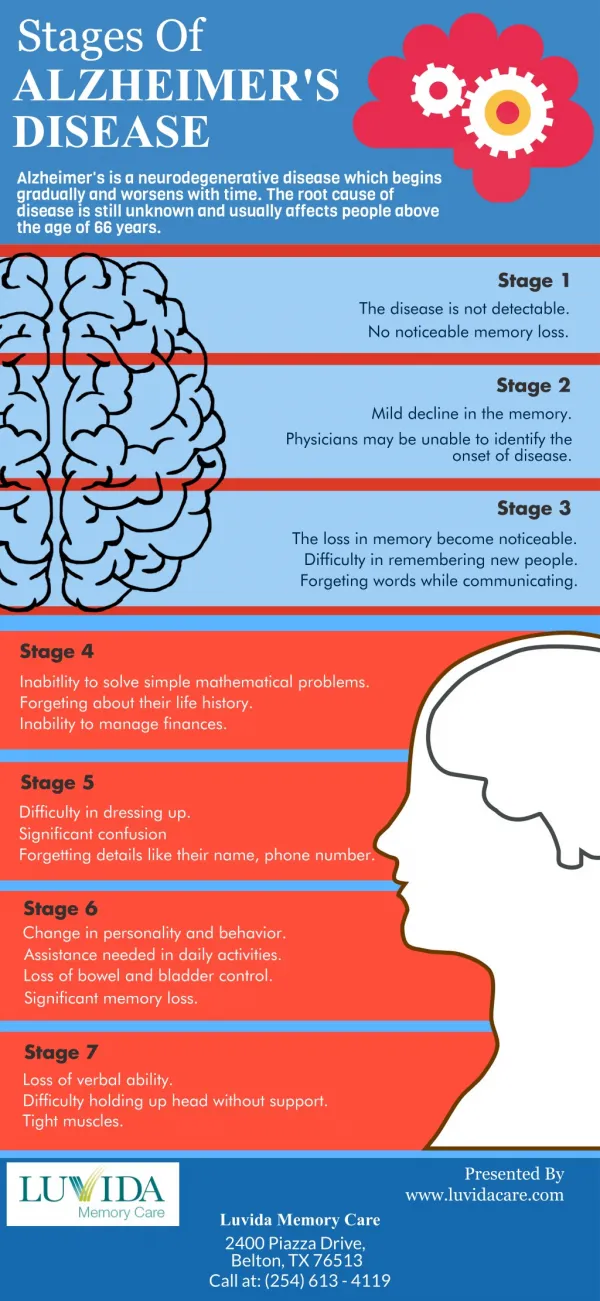
Learn about improving quality of life for persons with Alzheimer's disease, palliative care, healthcare models for older adults with dementia, and undertreatment of pain.

E N D
Improving Quality of Life for Persons with Alzheimers Disease R. Sean Morrison, MD Hermann Merkin Professor of Palliative Care Professor of Geriatrics and Medicine Vice-Chair for Research Brookdale Department of Geriatrics Mount Sinai School of Medicine New York, NY, USA
The Needs of an Aging Population Palliative Care: A New Model of Healthcare Improving Care for Older Adults with Dementia
Median Life Expectancy in Years Modern Sanitation Modern Medicine Antibiotics
Longevity in 2006 • Median age of death is 78 years. • Among survivors to age 65, median age at death is 82 years. • Among survivors to age 80, median age at death is 88 years
Number of Canadian Age 65 and Over with Disabilities Human Resources and Social Development Canada, 2005, www.hrsdc.gc.ca
Prevalence of Alzheimer’s Disease in Canadians Over Age 65 Canadian Study on Health & Aging
Leading Causes of Death in the U.S.: 2004 • Heart disease: 27% • Malignant neoplasm: 23% • Cerebrovascular disease: 6% • Chronic lung disease: 5% • Accidents: 5% • Diabetes: 3% • Alzheimer’s Disease 3% Account for 77% of all deaths Natl. Ctr. Health Statistics, CDC, 2007
Alzheimers & Related Dementias • Affects 30-40% of patients over 85 (50% in advanced stages) • Two thirds of newly admitted personal care residents have a diagnoses dementia • Currently costs 37,000 per year in caregiver, nursing home, and medication costs (5.5 billion dollars per year) • Projected 750,000 Canadians will suffer from advanced dementia by 2030 • There is no cure and disease modifying therapies are only marginally effective
The Burden of Dementia... • Financial and emotional costs to families and family caregivers • >90% have a family caregiver (>70% are women) • 20-40% of caregivers report depression • Caregivers reporting strain have a 1.5 fold increased risk of death • Decades of progressive dependency • Loss of work, family network, social supports, health, and savings. • Untreated physical symptoms
Undertreatment of Pain in Patients With Advanced Dementia • Prospective cohort study of 59 cognitively intact elderly patients with hip fracture and 38 patients with hip fracture and advanced dementia • Daily rating of pain by cognitively intact patients • Comparison of analgesic prescribing practices Morrison & Siu, JPSM, 2000
Analgesic Prescribing in Hip Fracture Patients with Advanced Dementia • 76% of cog. intact patients rated their average pre-operative pain as moderate-severe • 68% of cog. intact patients rated their average post-operative pain as moderate to severe Morrison & Siu, JPSM, 2000
Analgesic Dosing Schedules For Cognitively Intact and Dementia Patients Morrison & Siu, JPSM, 2000
Cognitive Impairment & Pain Management: Nursing Homes • Pain is documented less frequently for CI residents, even with similar numbers of painful diagnoses as less impaired residents (Sengstaken & King, 1993) • Less analgesic is prescribed/administered for CI residents, despite similar numbers of painful diagnoses (Horgas & Tsai, 1998) • Approximately ¼ of demented residents who were identified as having pain were receiving any analgesic therapy (Scherder et al, 1999; Bernabei et al, 1998; Won et al, 1999)
Sources of Suffering in Dementia - Pneumonia • 39 cognitively intact subjects asked to rate symptoms associated with pneumonia • Over 50% experienced at least one episode of severe dyspnea • 50% experienced moderate to severe anxiety • 40% experienced moderate to severe pain from coughing • 20% experienced severe nausea • Of 80 dementia patients hospitalized with pneumonia, 0 received treatment directed at any of the symptoms listed above Morrison & Siu, 2000
Sources of Suffering in Dementia – Iatrogenic Interventions • 165 cognitively intact adults hospitalized with acute medical illness • Subjects asked to rate pain and discomfort associated with common hospital procedures received by end-stage dementia patients • Ratings on a 0-10 cm visual analog scale Morrison et al, JPSM 1998
Severe (8-10) Arterial blood gas Moderate (4-7) Central line placement Nasogastric tube Peripheral IV insertion Phlebotomy Mild (1-3) IM/SC injection Urethral catheter Mechanical restraints Movement from bed to chair None (0) IV catheter Chest x-ray Vitals signs Transfer to a procedure Waiting for a test or procedure PO medications Pain Ratings For 16 Common Hospital Procedures For 165 Subjects Morrison et al, JPSM 1998
Severe (8-10) Nasogastric tube Mechanical ventilation Mechanical restraints Central line placement Moderate (4-7) Arterial blood gas Urethral catheter Mild (1-3) IV insertion Phlebotomy IV catheter IM/SC injection Waiting for procedures Movement from bed to chair Chest X-ray None (0) Transfer to a procedure Vitals signs PO medications Discomfort Ratings For 16 Common Hospital Procedures For 165 Subjects Morrison et al, JPSM 1998
Prevalence of Painful and Uncomfortable Procedures Morrison & Siu, JAMA, 2000
Other Sources of Suffering in Dementia • Loss of identity and personhood • Loss of control • Loss of meaning and purpose • Burden on loved ones (physical, financial, emotional, spiritual)
Care For for the Seriously Ill at the Turn of the Century (2000) • Unprecedented gains in life expectancy: exponential rise in number and needs of frail elderly • Cause of death shifted from acute sudden illness to chronic episodic disease • Untreated physical symptoms • Unmet patient/family needs • Disparities in access to care • An strained health care system facing enormous and increasing expenditures
94 y/o with severe congestive heart failure, a systolic blood pressure of 100, and shortness of breath at rest or with mild exertion. She is treated with an ACE inhibitor, a beta blocker, and judicious use of diuretics. She is disoriented to time and place but recognizes her family although frequently cannot remember or confuses their names • Is this resident terminally ill?
Traditional Medicine D E A T H Life Prolonging/Curative Care End of Life Care (Hospice) Disease Progression
NHWG; Adapted from work of the Canadian Palliative Care Association & Frank Ferris, MD A New Vision of Health Care for Persons with Serious Illness Disease Modifying Therapy Curative, or restorative intent Life Closure Death & Bereavement Diagnosis Palliative Care Hospice
Palliative Care Programs: • Interdisciplinary care teams that aim to relieve suffering, improve quality of life, optimize function, and assist with decision making for patients with advanced illness and their families. • Provided simultaneously with all other appropriate medical treatment. NCP for Quality Palliative Care, 2004
What Do Palliative Care Programs Do? (“What’s in the Syringe?”) N=325 patients Manfredi et al, JPSM, 2000
The Beneficial Effects of Hospice for Patients/Families • National Mortality Follow-Back Survey* • Overall quality of care reported higher in hospice compared to hospitals, NH, home health services • Improved emotional support for decedents and their families* • Medicare claims data† • Wives of husbands receiving hospice services prior to death had lower 18 month mortality rates than bereaved wives of men not receiving hospice (4.9% vs 5.4) • Retrospective medical record review‡ • Nursing home residents receiving hospice services significantly more likely to receive pain assessment and opioid therapy in the last 48 hours of life *Teno et al, JAMA, 2004; †Christakis & Iwashyna, Soc Sci Med, 2003; ‡Miller et al, JPSM, 2003
The Beneficial Effects of Hospice for Patients/Families • Study of 54 relatives of patients who died in hospital while receiving palliative care consultation matched to 95 relatives of patients who died while receiving usual care • 65% of family members of patients receiving hospital reported that their emotional or spiritual needs were met as compared to 35% of UC patients’ family members (P=0.004) • 67% of PC patients’ family members reported confidence in one or more self-efficacy domains as compared to 44% of UC patients’ family members (P=0.03) Gelfman LP, Meier DE, Morrison RS, Presented at AAHPM Annual Meeting, 2007
Special Challenges of Providing Palliative Care for Persons with AD • Difficulty in finding meaning and value in caring for non-communicative patients • Loss of primary care providers that treated patients prior to the onset of their dementia • Lack of advocates/surrogates for dementia patients to help with decision making • 50% of dementia subjects admitted to hospital lacked a functioning surrogate who could consent for medical treatment (Baskin et al, JAGS, 1998)
What Can We Do? • Integrate life prolonging care with care focused on comfort with a continual re-evaluation as to how to optimize quality of life and meet changing goals of care
Cure of disease Avoidance of premature death Maintenance or improvement in function Prolongation of life Relief of suffering Quality of life Staying in control Preserving dignity Support for families and loved ones Potential Goals of Care:
Where do we go from here? • Integration of life prolonging care with care focused on comfort with a continual re-evaluation as to how to optimize quality of life • Promotion of advance care planning in early stages of cognitive impairment with focus on goals of care and acceptable quality of life • Not medical interventions • Focused efforts on identifying and treating distressing symptoms • Efforts focused on developing palliative care within long-term care settings
National Consensus Project on Quality Palliative Care • Mission: To create a set of voluntary clinical practice guidelines to guide the growth and expansion of palliative care in the United States • Clinical Practice Guidelines: In the absence of organized programs or specialists, guide clinicians to incorporate vital aspects of palliative care into their practice to improve care for their sickest patients, over the course of their illnesses
NCP Clinical Practice Guidelines Domains • Structure and Process of Care • Physical • Psychological and Psychiatric • Social • Spiritual, Religious and Existential • Cultural • The Imminently Dying Patient • Ethics and Law
What Can You Do? • Health care organizations: Use the guidelines to start a palliative care program for efficient, effective management of your sickest patients • Clinicians: Ask for a palliative care program applying these guidelines in support of your care; or, in the absence of a program, use standards to provide core elements to care of sickest patients
What Can You Do? • Palliative care advocates: Champion adoption and use of guidelines in your organization & field and share with colleagues • Patients and families: Choose health care organizations and providers who have adopted clinical practice guidelines, and ask for a palliative care consult when you are facing advanced chronic or life-threatening illness
National Consensus Project Voluntary Clinical Practice Guidelines for Quality Palliative Care For more information: www.nationalconsensusproject.org
Although the world is full of suffering, it is also full of the overcoming of it. Helen Keller, Optimism 1903