Download
1 / 39
400 likes | 950 Vues
Managing high blood pressure in acute stroke: The ‘Efficacy of Nitric Oxide in Stroke’ (ENOS) trial. Philip Bath Chief Investigator Version 1.0. From bench to patient to population. Epidemiology IST/TAIST/BASC Pre-clinical: experimental Nitric oxide donors

E N D
Managing high blood pressure in acute stroke: The ‘Efficacy of Nitric Oxide in Stroke’ (ENOS) trial Philip Bath Chief Investigator Version 1.0
From bench to patient to population Epidemiology IST/TAIST/BASC Pre-clinical: experimental Nitric oxide donors Pre-clinical: meta-analysis Nitric oxide donors Phase I, human volunteers SNP SPECT trial Phase II, dose escalation, safety GTN/Xenon CT trials Clinical: meta-analysis Cochrane Library Phase III, safety and efficacy ENOS trial Clinical: meta-analysis Cochrane Library
SBP in acute ischaemic stroke: IST High blood pressures is very common in acute ischaemic stroke affecting ~80% of patients N=17,398 Leonardi-Bee et al. Stroke 2002;33:1315-20
High blood pressure in acute stroke BP falls over the first 1-2 weeks (in 2/3 patients) BP levels are very variable during this time See example patient with acute stroke
Systolic BP & outcome: IST Both low and high BP are associated independently with early death and late death/disability N=17,398 Leonardi-Bee et al. Stroke 2002;33:1315-20
SBP & early recurrence: TAIST High blood pressure is associated with an increased risk of early recurrence after ischaemic stroke 10 N=1,384 Sprigg et al. J Hypertension 2006;24:1413-17
To lower or not lower BP in acute stroke An old debate! Arch Neurology 1985;42:999-1002
Guidelines are expert-based, Encephalopathy, heart failure/ischaemia, aortic dissection Other hypertensive stroke patients not evidence-based Reduce BP Do not lower: BP at all SBP below 160 Reduce: if SBP>200-220 if DBP>120-130 to MBP=120-140 MBP by < 20% Guidelines for management
Completed randomised trials Class Intervention N/C Inclusion Outcome Trial ACE-i Perindopril 24/1 S170-250; 7d TCD Dyker ACE-I Lisinopril 38/1 1d BP Eveson ARA Candesartan 339/+ IS, S>200; 3d Vasc. event ACCESS ARA Losartan 24/1 M110-145 BP, SPECT CBF Nazir (ß-RA Atenolol/prop 358/1 2d Disability BEST) CCB Nicardipine 16/1 IS; S>170; 3d CBF (SPECT) Lisk (CCB Nimodipine 295/+ IS; 1d ADL (BI) INWEST) CCB Nimodipine 19/? IS; ?d Dose Fagan CCB Nimodipine 90/1 1d iv/po Uzuner Diur. Bendroflu. 40/1 4d BP Potter NO GTN 37/1 5d BP, platelets Bath NO GTN 90/1 S100-230; 4d BP, dose Rashid NO GTN 18/1 S140-220 BP, xenon CBF Willmot SANS Phenylephrine 15/1 D/P mismatch Lesion vol. Hillis Blood pressure in Acute Stroke Collab. (BASC) II. Cochrane Library
Candesartan vs. placebo for 7 days (then candesartan for all for 1 year) 500 patients - trial stopped early after 339 for ‘safety’ SBP>200 and/or DBP>110; or 2x >180 and/or >105 Conscious, motor weakness, <72 hours No effect on BP? No effect on functional outcome at 3 months (primary outcome) Reduced vascular events at 1 year ACCESS Schrader et al. Stroke 2003;34,1699-1703 N=339
CCB in acuteischaemic stroke: No effect on outcome CCBs: Horn & Limburg. Cochrane Library 2002
Multimodality of drugs BP modifying drugs have other actions: ACE-I Neuroprotection, block tissue effects, (antiplatelet) ARA Neuroprotection, block tissue effects ß-RA Antiplatelet, negative inotrope CCB Antiplatelet, negative inotrope, ‘cerebral steal’ NO Neuroprotection, cerebral vasodilator, anti-platelet, (antileucocyte) SANS Inotrope, chronotrope, vasoconstrictor, platelet agonist Bath P. Stroke 2003;34:1334-5
Prior hypertension 50% of patients are on antihypertensive medication before stroke Should we continue or stop these during acute phase of stroke? • Continue • Lower blood pressure with potential benefits/hazards? • ‘Beneficial’ drug classes: ACE-I, ARA, NO ? • ‘Detrimental/neutral’ drug classes: CCBs, ß-RA ? • Administration in presence of dysphagia • Prior non-compliance -> massive fall in BP • Stop temporarily • ‘Rebound’ rise in BP? • Remember to re-start for secondary prevention • No completed trials
Ongoing/planned trials There are several large ongoing trials of antihypertensive agents in acute stroke: Rx N aim C aim N now C now Inclusion Outcome Trial Continue 2900 100+ 530 26 IS/PICH + HT mRS COSSACS vs. stop 2500 200+ 290 34 IS/PICH + HT mRS ENOS GTN 5000 200+ 680 36 IS/PICH + HT mRS ENOS (Telmi- 20000 640 20133 644 IS + 120-180 stroke PRoFESS) sartan Cande- 2500 100+ 886 79 IS/PICH + HT mRS SCAST sartan stroke ‘Usual’ 400 70 300+ ? PICH + HT mRS INTERACT-p 3000 PICH + HT mRS INTERACT
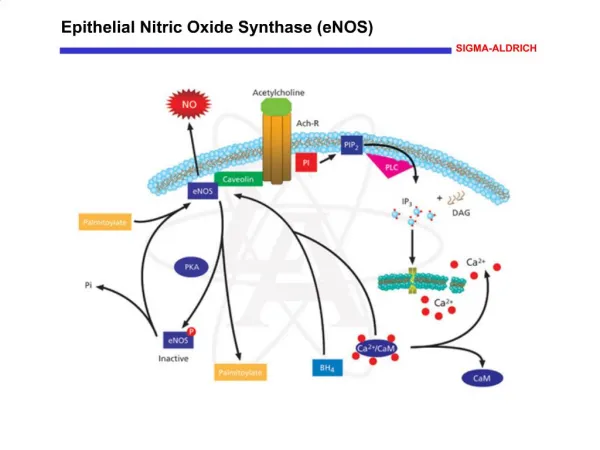
NO path Rashid et al. J Stroke Cerebrovasc Dis 2003;12:82-7
NOx levels low in stroke Low levels associated with a poor outcome Supplementing NO might improve outcome? Nitric oxide (NOx) levels in acute stroke * ** ** Rashid et al. J Stroke Cerebrovasc Dis 2003;12:82-87
Experimental stroke NO donors: Reduce lesion size Increase regional CBF NO is neuroprotective? NO in stroke Willmot et al. Nitric Oxide 2005;12:141-9
Cerebral autoregulation Cerebral perfusion normally maintained independently of BP Curve right-shifted in chronic high BP Autoregulation lost following stroke Local perfusion becomes dependent on BP Strandgaard et al. Br Med J 1973 Barry & Lassern. J Hypertension 1984
Glyceryl trinitrate (GTN): left infarct BP lowered by 10% with GTN; CBF measured using xenon CT CBF: Perfusion did not fall N=18 Willmot et al. Hypertension 2006;epub
GTN: left haemorrhage And the same in primary intracerebral haemorrhage N=18 Willmot et al. Hypertension 2006;epub
Transdermal glyceryl trinitrate (NO donor) on BP in acute stroke GTN lowers BP in acute stroke (measured using ambulatory BP measuring [ABPM]) N=37 Bath et al. Cerebrovasc Dis 2001;11:265-72
Transdermal glyceryl trinitrate (NO donor) in acute stroke • Acute stroke (<96 hours) • Ischaemic or haemorrhagic stroke • GTN (7 days): 5mg; 5 mg for 4d then 10mg; 10 mg Day 1 Control GTN p Subjects 30 60 Mean BP (mmHg) 110.5 104.3 <0.001 MCA velocity (m/s) 26.3 24.6 NS Pulsatility index 1.42 1.41 NS Augmentation index 132.7 115.7 <0.001 GTN: Lowered BP Did not alter middle cerebral artery blood flow velocity Reduced augmentation index, i.e. increases aortic compliance N=90 Rashid et al. J Stroke Cerebrovasc Dis 2003;13:143-51
GTN on blood pressure GTN lowered systolic BP (systematic review): • Top: Measured over 24 hours (ABPM) • Bottom: Measures 2 hours after placement of GTN Gray et al. J Stroke Cerebrovasc Dis 2006;15:245-9
Efficacy of Nitric Oxide inStroke (ENOS) • Assess if lowering blood pressure improves outcome • Interventions (for 7 days): • Transdermal glyceryl trinitrate (5 mg daily) or control • Continue / stop prior antihypertensive therapy • Ischaemic or haemorrhagic stroke within 48 hours • 5,000 patients • Internet: Randomisation, data collection, trial management • 711 patients, 41 centres, 13 countries, 4 continents (1/7/07) • Start-up funding by Hypertension Trust, BUPA Foundation • Main phase funding by MRC Nov 2006-Oct 2011 www.enos.ac.uk/
ENOS: Aims / interventions 1. Does acute lowering of BP with GTN reduce death and dependency? • GTN 5mg daily versus nothing for 7 days 2. Should prior antihypertensive medication be continued or temporarily stopped during the acute phase of stroke? • Continue versus stop prior treatment for 7 days On top of standard evidence-based acute medical and nursing care, and secondary prevention www.enos.ac.uk/
ENOS: Outcomes Primary (3 months): • Modified Rankin Scale: 0-2 versus 3-6 Secondary outcomes: • Efficacy: disability, institutionalisation, early recurrence, QoL, mood, cognition • Safety: death, deterioration, CT lesion size Primary outcome in sub-groups: • Ischaemic, haemorrhagic stroke • Systolic BP levels (mmHg): 140-160, >160 • Timing of treatment (hours): <12, 12-48 www.enos.ac.uk/
ENOS: Sample size Assumptions: • Alpha 5% • Power 90% • Control rate for mRS>2 50% • GTN rate for mRS>2 45% • Absolute treatment effect 5% • Losses to follow-up 5% • 5000 patients • Analysis by intention-to-treat www.enos.ac.uk/
Canada (Portugal) UK Belgium Poland Italy (Russia) China/ Hong Kong (USA) (Spain) (Greece) (Thailand) (Mexico) (Nigeria) (Egypt) (India) Singapore Philippines New Zealand (Colombia) (Brazil) (South Africa) Sri Lanka (Malaysia) Australia
ENOS is world’s first acute stroke trial to use the internet for randomisation and data collection
ENOS: Baseline GTN/no GTN Continue/stop Subjects 659 297 Age (mean) 69 70 Male (%) 57 53 Recent nitrate (%) 6 11 Prior high BP (%) 67 93 SBP (mmHg) 168 167 AF (%) 11 15 Severity (SSS) 38 39 Time < 24h (%) 31 29 www.enos.ac.uk/
ENOS: Stroke type Non-adjudicated information from investigator: Ischaemic 82% Haemorrhage 14% www.enos.ac.uk/ N=646
ENOS: Outcomes, day 7 % GTN/no GTN Continue/stop Death 2.5 0.7 Recurrence 1.9 2.4 Infarction 1.1 1.7 Haemorrhage 0.5 0.3 Unknown 0.3 0.3 Deterioration 7.7 6.1 SNSS (/58) 45 46 (at baseline 38 39) www.enos.ac.uk/ N=646/293
ENOS: Rankin, day 90 Planned mRS >2 = 50% Current mRS >2 = 48% Current mRS >2 = 45% www.enos.ac.uk/ N=573/258
Systolic BP (mmHg) World Congress of Neurology 2005 P=0.002 N=168
ENOS: Sub-studies • MR substudy • Chris Chen, Singapore, funded 1/05 • Lawrence Wong, Kong Kong, submitted for funding • GTN on lesion volume, diffusion, perfusion • CT substudy • GTN on lesion volume, recurrence • Pharmacogenetics • GTN effects on BP by genotype, e.g. eNOS • Surrogate markers of efficacy • GTN on serum biomarkers, e.g. NSE & S-100 • …
ENOS in China National Coordinating Centre: Tiantan, Beijing Local centres: Patients • Beijing, Tiantan 16 • Hong Kong 4 • Wenzhou 67 China Rest Number 87 615 Age 64 70 Male (%) 71 55 Scandinavian Stroke Scale (/57) 35 35 Intracerebral haemorrhage (%) 49 11 mRS (mean) 2.4 2.7
ENOS: ‘streamlined’ • Melds with other trials: hyperacute, high-tech • Wide time-window, 1-48 hours • Ischaemic and haemorrhagic stroke • Any clinical syndrome, pathophysiology • Can be given with rt-PA (nitrates in NINDS!) • Easy intervention: transdermal / dysphagia • Can be led by nurses • Modest data collection: days 0, 7, 90 (SAE) • Internet randomisation / data registration • ASTN, CSC, UKSRN approved • This trial needs you! www.enos.ac.uk/
Source: The Stroke Association Time of some staff University of Nottingham Website/database The Hypertension Trust Xenon CT sub-study BUPA Foundation Start-up phase Medical Research Council Main phase (from 1/11/6) Funding
Thanks Questions?