Download

1 / 68
920 likes | 2.38k Vues
PROTEIN ENERGY MALNUTRITION. DEFINITION. ‘ A state of nutrition in which a deficiency (or imbalance) of energy, protein & other nutrients causes measurable adverse effects on tissue/body structure & function & clinical outcome ’. MAGNITUDE OF PROBLEM - INDIA.

E N D
DEFINITION ‘A state of nutrition in which a deficiency (or imbalance) of energy, protein & other nutrients causes measurable adverse effects on tissue/body structure & function & clinical outcome’
MAGNITUDE OF PROBLEM - INDIA • % of Underweight <5yrs (moderate) 47 • % of Underweight <5yrs (severe) 18 • % of Wasting <5yrs- 16 (moderate & severe) • % of Stunting <5yrs- 46 (moderate & severe) These data are based on NFHS2 findings
BASIS OF CLASSIFICATION • Weight - for – Age • Weight- for – Age & Edema • Weight – for – Height & Height-for-age • SD Scores • Mid-arm Circumference
CLASSIFICATION BASED ON WEIGHT FOR AGE IAP CLASSIFICATION OF MALNUTRITION
WELLCOME - TRUST CLASSIFICATION CLASSIFICATION BASED ON WEIGHT- FOR AGE & EDEMA
CLASIFICATION BASED ON WEIGHT-FOR-HEIGHT & HEIGHT-FOR-AGE WATERLOW CLASSIFICATION
CLASSIFICATION BASED ON SD SCORES WHO CLASSIFICATION OF MALNUTRITION
CLASSIFICATION BASED ONMID-ARM CIRCUMFERENCE Technique Between 1-5 yrs constant 16.5-17.5 cms
Conditioning influences Low birth weight Infections - eg. Diarrhoea, Respiratory infections, Measles / Whooping cough, Tuberculosis, Helminthiasis Socio economic factors Poverty Ignorance Illiteracy Lack of knowledge regarding food values Unhygienic environment Large family size Over crowding Cultural practices Food habits Customs and belief Tradition Religion Food fads (personal likes & dislikes) Cooking practices Child rearing practices Superstious belief ECOLOGY OF MALNUTRITION
THEORIES OF MALNUTRITION • Protein deficiency • Toxic theory • Niacin theory • Increased ferritin level • Dr.Gopalan’s dysadaptation theory • Free radical theory • Aflatoxin poisoning New theory
FREE RADICAL THEORY • Free oxygen radicals potentially toxic to cell membrane and are produced during various infections • These oxides are normally buffered by proteins and neutralised by antioxidants such as Vit.A, C & E and selenium • In malnourished child deficiency of these nutrients in the presence of infection or aflatoxin may result in the accumulation of toxic – free oxygen radicals • These may damage liver cells giving rise to Kwashiorkor
FREE RADICAL THEORY OF KWASHIORKOR Noxae Inadequate protective pathway Free Radicals Fe Catalyzed Macro molecular damage Malnutrition Inadequate Repair Fatty Liver
AFLATOXIN POISONING Noxae Low protein diet growth stops Stunting Very low protein Anorexia Marasmus Insufficient diet weight loss wasting (marasmic kwashiorkar) DIET Kwashiorkar
SPECTRUM OF PEM • Underweight • Kwashiorkar Welcome classification • Marasmus • Marasmic Kwashiorkar • Prekwashiorkar - features of Kwashiorkor no edema • Nutritional dwarfism – Stunting but not wasting, Micronutrient deficiency cause for stunting • Invisible PEM – Age 6 – 24 months, looks entirely normal but too small for age, growth chart best way to identify
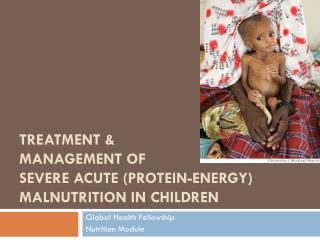
MARASMUS • Severe wasting of muscle & s/c fats • Severe growth retardation • No edema or hair changes or fatty liver • Alert but miserable • Hungry
Cardinal features Oedema Psychomotor changes Growth retardation Muscle wasting Associated features Moon face Hair changes Skin changes Depigmentation Anemia Hepatomegaly Flaky paint dermatitis Cardiac failure Dehydration Vitamin deficiencies KWASHIORKOR
MARASMIC KWASHIORKOR • Syndrome seen in marasmic children, with severe muscle & fat wasting who suddenly develop oedema, due to increased protein deficiency than before. • Thus clinical features, combination of Marasmus & Kwashiorkor . • Anemia is moderate & one/ more Vitamin deficiencies may be evident.
INFECTION & IMMUNITY IN PEM • Infection & Immunity interrelated to PEM • Infectious disease worsens in PEM & vise versa PEM usually weakens resistance to infection, when worsens results in high mortality among toddlers & under 5 children • These children may present with episodes of acute infection or recurrent chronic insidious infection may go undetected unless specifically looked for i.e. Recurrent attacks of diarrhoeal diseases, pneumonia, septicaemia, measles, tuberculosis and malaria common, Urinary tract infection often occur but may go undetected, have to be suspected. • Intestinal parasitosis ascariasis, ankylostomiasis & Giardiasis frequent • All these impair nutritional status leading to growth retardation & frank PEM & contribute to high mortality
IMMUNITY • Humoral : Ig G, IgM & Secretory Ig A not significantly affected in mild to moderate PEM, hence host respond well to bacterial challenges & viral vaccines. • But depressed in severe PEM with infections • Cell Mediated Immunity (CMI) : is impaired in all grades of PEM except Gr I, severely impaired in G III & Gr IV PEM & Kwashiorkor • This explains –ve Tuberculin test in Marasmus & Kwashiorkor in spite active TB • Following dietary treatment when the pt. improves, T Test may convert to +ve. • Serum C reactive Protein & Complement C3 are depressed in severe PEM, but rise in presence of infection & behave as acute phase reactants.
Tests that may be useful Blood glucose Peripheral smear Hemoglobin Urine Examination Stool Examination Chest X-ray Mantoux Tests that are of little or no value Serum proteins Electrolytes HIV INVESTIGATIONS
COMPLICATIONS • Hypoglycemia • Hypothermia • Infections (bacterial, viral & fungal) • Hypokalemia • Hyponatremia • Dehydration & shock • Heart failure
CRITERIA FOR ADMISSION COMPLICATED • <6 months or • > 6 months but not fulfilling the criteria for uncomplicated also considered "complicated". • Institutional care is considered mandatory UNCOMPLICATED • > 6 months of age • alert • preserved appetite, • clinically assessed to be well • living in a conducive home environment.
WHO GUIDELINES FOR THE IN-PATIENT TREATMENT OF SEVERELY MALNOURISHED CHILDREN
MANAGEMENT A. General principles for routine care (the’10 steps’) B. Emergency treatment of shock and severe anemia C. Treatment of associated conditions D. Failure to respond to treatment E. Discharge before recovery is complete
GENERAL PRINCIPLES FOR ROUTINE CARE • These steps are accomplished in two phases: • an initial stabilization phasewhere the acute medical conditions are managed; and • a longer rehabilitation phase. • Note that treatment procedures are similar for marasmus & kwashiorkor.
STEP 1. TREAT/PREVENT HYPOGLYCAEMIA • Blood sugar level <54 mg/dl or 3 mmol/L • Assume hypoglycemia when levels cannot be determined. • CONSCIOUS CHILD- 50 ml bolus of 10% glucose by nasogastric (NG) tube. • UNCONSCIOUS CHILD, lethargic or convulsing -IV sterile 10% glucose (5ml/kg), followed by 50ml of 10% glucose or sucrose by NG tube. • Start two-hourly feeds, day and night
STEP 2. TREAT/PREVENT HYPOTHERMIA • If axillary temperature <35oC, take rectal temperature • If the rectal temperature is <35.5oC (<95.9oF): • rewarm the child: either clothe cover with warmed blanket & place a heater or lamp nearby or put the child on the mother’s bare chest (skin to skin) and cover them – Kangaroo mother care • feed straightaway
STEP 3.TREAT/PREVENT DEHYDRATION • Difficult to estimate dehydration using clinical signs alone • Assume all children with watery diarrhea may have dehydration • Do not use the IV route for rehydration except in cases of shock • Continue feeding
ASSESSMENT OF DEHYDRATION IN SEVERELY MALNOURISHED CHILDREN Basic format remains the same Some signs unreliable • Mental state • Mouth, tongue and tears • Skin turgor Edema and hypovolemia can coexist
DIAGNOSIS OF DEHYDRATION IN SEVERELY MALNOURISHED CHILDREN • History of diarrhea ( with large volume of stools) • Increased thirst • Recent sunken eyes • Prolonged CFT, weak/absent radial pulse, decreased or absent urine flow Difficult using clinical signs alone Best to assume that all with watery diarrhea have some dehydration Treat with ORS unless shock is present
WHICH ORS SHOULD BE USED IN SEVERE MALNUTRITION? • OPTIONS • Low osmolarity ORS with potassium supplements • ReSoMal (not available in India)IAPendorses the use ofLOW OSMOLARITY WHO ORSfor all types of diarrhea and nutritional status for logistics and programmatic advantages.
STEP 4. CORRECT ELECTROLYTE IMBALANCE • Plasma sodium may be low though body sodium is usually high. Sodium supplementation may increase mortality. • Potassium & Magnesium are usually deficient and needs supplementation;may take at least two weeks to correct. • Edema if present is partly due to these imbalances. Do NOT treat edema with a diuretic
STEP 5. TREAT/PREVENT INFECTION • Usual signs of infection, such as fever, are often absent. Give broad spectrum antibiotics to all. • Hypoglycemia/hypothermia usually coexistent with infection. Hence if either is present assume infection is present as well • No complications - Co-trimoxazole • Severely ill - Ampicillin + Gentamicin • If the child fails to improve clinically within 48 hours, add: cefotaxime/ceftrioxone
STEP 6. CORRECT MICRONUTRIENT DEFICIENCIES • All severely malnourished children have vitamin and mineral deficiencies • Vitamin A orally on Day 1 • Give daily : • Multivitamin supplement • Folic acid 1 mg/d (give 5 mg on Day 1) • Zinc 2 mg/kg/d • Iron 3 mg/kg/d after first week
COMPOSITION OF ELECTROLYTE MINERAL SOLUTION FOR SEVERELY MALNOURISHED CHILDREN Ingredient Mass (g) mmol per 20 ml Potassium chloride (KCl) 224 24 Tripotassium citrate 81 2 Magnesium chloride (MgCl2.6H20) 76 3 Zinc acetate (Zn accetate.2H20) 8.2 0.3 Copper sulphate (CuSO4.5H20) 1.4 0.045 • To be added to diet or oral rehydration salts solution. • Add 20 ml of the solution to a litre of diet or oral rehydration salts. However, appropriate Vitamin mineral mix is not available in India. In this scenario, one may use combinations of various commercial preparations available
STEP 7. START CAUTIOUS FEEDING • Small, frequent feeds • Oral or nasogastric (NG) feeds (never parenteral preparations) • Milk-based formulas such as starter F-75 containing 75 kcal/100 ml and 0.9 g protein/100 ml will be satisfactory for most children • 130 ml/kg/d of fluid (100 ml/kg/d if the child has severe edema) • If the child is breastfed, encourage to continue breastfeeding
STEP 7. START CAUTIOUS FEEDING • A gradual transition is recommended to avoid the risk of HEART FAILURE. • Monitor during the transition for signs of heart failure • If respirations increase by 5 or more breaths/min & • pulse by 25 or more beats/min for two successive 4-hourly readings, reduce the volume per feed
STEP 8. ACHIEVE CATCH-UP GROWTH • Readiness to enter the rehabilitation phase is signaled by a RETURN OF APPETITE, usually about one week after admission • Recommended milk-based F-100 contains 100 kcal & 2.9 g protein/100 ml • In rehabilitation phase vigorous approach to feeding is required to achieve very high intakes & rapid weight gain of >10 g gain/kg/d
TO CHANGE FROM STARTER TO CATCH - UP FORMULA • Replace starter F-75 with the same amount of catch-up formula F-100 for 48 hours then, • Increase each successive feed by 10 ml until some feed remains uneaten. • The point when some remains unconsumed is likely to occur when intakes reach about 30 ml/kg/feed (200 ml/kg/d)
STEP 9. PROVIDE SENSORY STIMULATION AND EMOTIONALSUPPORT • Delayed mental and behavioral development is present • Provide: • Tender loving care • Cheerful, stimulating environment • Structured play therapy 15-30 min/d • Physical activity as soon as the child is well enough • Maternal involvement when possible (e.g. Comforting, feeding, bathing, play)
STEP 10. PREPARE FOR FOLLOW-UP AFTER RECOVERY • A child who is 90% weight-for-length (equivalent to -1SD) can be considered to have recovered • Show parent or caregiver how to: • Feed frequently with energy - and nutrient-dense foods • Give structured play therapy • Advise parent or caregiver to: • Bring child back for regular follow-up checks • Ensure booster immunizations are given • Ensure vitamin A is given every six months