Download
1 / 48
480 likes | 496 Vues
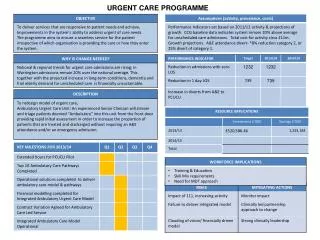
This article discusses the organization of urgent care in Acute Medicine and provides strategies to reduce pressure on beds, improve patient flow, and enhance clinical quality indicators. It also explores the role of the GP Assessment Unit and the impact of percutaneous endoscopic gastrostomy on patients with dementia.

E N D
Acute Medicine - Organisation of Urgent Care Dr Kevin Jones FRCP MD Royal Bolton Hospital
Urgent Care • “The number one issue facing the NHS in England is reversing the ‘unsustainable’ rise in emergency hospital admissions .... There has been an almost 12 per cent rise in admissions over the last five years” • Nuffield Trust, 2010
Acute Medical Unit Assessment and Short Stay Beds D1 Ward - female (26 beds) D2 Ward - male (22 beds ) GP Assessment Unit (GPAU) Clinical Decisions Unit (CDU) Emergency Department Bolton Community Unit (BCU) DVT Clinic
GP Assessment Unit • In Main Outpatients (Blue Bay) • Same area as SARC Clinic • Purpose Built Ambulatory Area • Next to Emergency Department • Next to CDU ( Red Area ) • Acute Medicine Consultant 0800-1600 • Closed weekends and bank-holidays • In January 2013 – average 8 patients/day
Clinical Decisions Unit (CDU) • Purpose built in Red Area of Outpatients • Not strictly speaking a CDU • Only 14 beds • Used as an ultra-short stay unit (12 hrs ideal) • Telemetry and monitoring • Cardiac chest pains awaiting Troponin-I • Acute Medicine Consultant 0800-1600 hrs
Clinical Decisions Unit (CDU) • February 2013 • 254 admissions ( 9/day ) • 82% discharged home • Only 35% with length of stay < 12 hours • 33% staying longer than 24 hours
Clinical Decisions UnitRing fencing • June 2013 • In last 2 weeks – 186 admissions • 13 per day • 88% discharged home
Admissions(January 2013) D1 448 D2 442 CDU 254 GPAU 173 Mean 42 per day 45% discharged directly home from AMU
Time of Admission to AMU Approximately 24% total admissions come direct from GPs Do our rotas reflect our demand and support senior review?
Discharge Flow does not mirror ‘input’ flow, and lags behind
Lengths of Stay for AMU discharges 45% discharged home 55% admitted to specialist ward 75% of patients kept on Acute Medical Unit are discharged within 24 hours
How to ReducePressure on Beds • Maintain 85% bed occupancy • Reduce Lengths of Stay • Consultant-held Triage Bleep • Early senior decision maker review • Capacity for Short Stay in AMU • Ambulatory Care
Consultant held Triage Bleep for GP Direct • Results • Mean number of calls dealt with per day between 0800 and 1600: 13 (range 8 – 23) • On average the consultant is able to divert or deflect 4 – 6 admissions per day. • Giving advice to the GP • Advising referral to a specialist clinic • Giving the patient an appointment in GPAU • Asking the hospital Referral and Assessment Team to assess patients with social problems.
Triage Bleep - Advice • Subarachnoid haemorrhage • Temporal arteritis • Transient ischaemic attack • Bell’s Palsy • Pneumonia • Atrial Fibrillation • Hyperkalaemia • Severe Hypertension • Iron Deficiency Anaemia
GP Assessment UnitMain Referrals Headaches Chest pain Shortness of breath Blackouts and collapses Generally unwell
Emergency Admissions Length of Stay • Greater Manchester (12 Trusts) • Range 1.8 to 3.8 days • Mean 2.6 days • Bolton 2.4 days
95% Emergency Dept Target • >95% for every month April to Dec 2012 • Below 95% for January 2013 • Above 95% for February 2013 • 95.6% for March 2013 • 95.5% for Quarter 4 • 96.9% Year to Date
Clinical Quality Indicators for Acute Medical Units • 1. All patients admitted to the AMU should have an early warning score measured upon arrival on the AMU. • 2. All patients should be seen by a competent clinical decision maker within 4 hours* of arrival on the AMU who will perform a full assessment and instigate an appropriate management plan. • 3. All patients should be reviewed by the admitting consultant physician or an appropriate speciality consultant physician within 14 hours of arrival on the AMU**.
Clinical Quality Indicators for Acute Medical Units • All acute medical units should collect the following data • Hospital mortality rates for all patients admitted via the AMU • Proportion of admitted patients who are discharged directly from the AMU • Proportion of patients discharged from the AMU who are readmitted to hospital within 7 days of discharge
Consultant held Triage Bleep GP Assessment UnitClinical Decisions Unit • Any Questions ?
Ambulatory Emergency Care • Acute Admissions from Care Homes • Acute Admissions from non-acute NHS beds • End of Life Care
Percutaneous Endoscopic Gastrostomy Does Not Prolong Survival in Patients With Dementia • Lynne M. Murphy, MSN, RN, CNSN; • Timothy O. Lipman, MD • Arch Intern Med. 2003;163(11):1351-1353.
Improving end of life care for nursing home residents: an analysis of hospital mortality and readmission rates. . • Ahearn DJ,Jackson TB, McIlmoyle J, Weatherburn AJ. • Postgrad Med J. 2010 Mar;86(1013):131-5
Ahearn DJ et al, 2010 • Analysis of all admissions to the acute medical unit of a busy district general hospital over a 94 day period, comparing nursing home residents with all admitted patients aged over 70 years.
Ahearn DJ et al, 2010 • Nursing home residents were significantly less likely to survive the admission than elderly people living in the community. • 33.9% of nursing home residents did not survive the admission • 51.6% died within 6 weeks of admission. • Of those discharged alive, 41.5% were readmitted or died within 6 weeks. • Patients with a higher level of comorbidity were less likely to survive the admission or live to 6 weeks.
Ahearn DJ et al, 2010 • Many nursing home residents find acute admission distressing, • Many hospital admissions are ‘inappropriate’. • Advance care planning can improve patients’ end of life care. • Nursing home residents were significantly less likely to survive acute medical admission than elderly people living in the community.
Ahearn DJ et al, 2010 • Patients with a higher level of comorbidity are less likely to survive the admission or to 6 weeks than those with lower levels. Advance care planning should be considered in all nursing home residents, especially those with the greatest level of comorbidity. • Postgrad Med J 2010;86:131-135.
Is it a TIA or not? • Are the neurological symptoms focal rather than non focal? • Are the neurological symptoms negative rather than positive? • Was the onset of the focal neurological symptoms sudden? • Were the focal symptoms maximal at onset? • Syncope does not occur with TIA
TIA – ABCD2 Score • Age > 60 yrs 1 • BP > 140/90 1 • Clinical Weakness 2 • Speech 1 • Duration < 1 hour 1 • > 1 hour 2 • Diabetes 1
TIA – ABCD2 Score • Start aspirin 300mg • Score 4 or more – clinic within 24 hours • Score less than 4 – clinic within 1 week
Hypertensive Urgency Systolic > 200 mmHg Diastolic > 120 mmHg No symptoms ( headache ) No end-organ damage Usually poorly compliant
Subarachnoid haemorrhage • Suddeness of onset more important than severity • Comes on to maximum intensity within a minute • Lasts for at least an hour
Stanley et al, Lancet, 373, Jan 3rd 2009. Glasgow-Blatchford
Pneumonia – BTS Guidelines • Can be a clinical diagnosis • Chest X-ray not essential • CRB-65 score of 0-1 may be treated in the community
Pneumonia – CURB 65 score • Confusion – new onset • Urea > 7.0 mmol/l • Respiratory rate > 30 / min • BP - < 90 syst or < 60 diast • Age > 65 yrs
Bell’s Palsy • Diagnose lower motor neurone palsy • Imaging not required unless atypical or not recovering after 8 weeks • Give prednisolone 60 mg for 1 week • Protect the eye • Primary care – not acute medicine
Temporal Arteritis • Usually aged above 50 years • ESR usually above 80 mm/hr • Start prednisolone 60 mg daily • Temporal artery biopsy within a week