Download
1 / 1
10 likes | 184 Vues
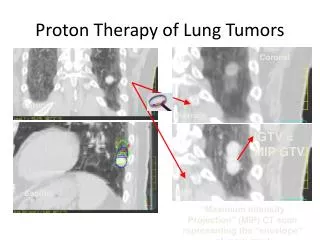
Increased Local Control of Lung and Liver Tumors Associated with Dose-Escalated Stereotactic Body Radiation Therapy (SBRT) Supports a Dose-Response Relationship Robert McCammon, MD, Tracey Schefter, MD, Laurie Gaspar, MD, Rebekah Zaemisch, MD, Daniel Gravdahl, MD, Brian Kavanagh, M.D.

E N D
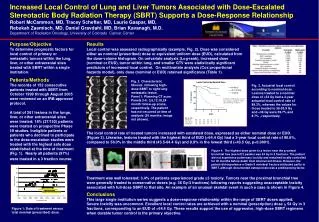
Increased Local Control of Lung and Liver Tumors Associated with Dose-Escalated Stereotactic Body Radiation Therapy (SBRT) Supports a Dose-Response Relationship Robert McCammon, MD, Tracey Schefter, MD, Laurie Gaspar, MD, Rebekah Zaemisch, MD, Daniel Gravdahl, MD, Brian Kavanagh, M.D. Department of Radiation Oncology, University of Colorado Cancer Center Purpose/Objective To determine prognostic factors for local control of primary or metastatic tumors within the lung, liver, or other extracranial sites treated with SBRT within a single institution. Results Local control was assessed radiographically (example, Fig. 2). Dose was considered either as nominal (prescribed) dose or equivalent uniform dose (EUD), calculated from the dose-volume histogram. On univariate analysis (Log-rank), increased dose (nominal or EUD), tumor within lung, and smaller GTV were statistically significant predictors of increased local control. On multivariate analysis (Cox proportional hazards model), only dose (nominal or EUD) retained significance (Table 1). Patients/Methods The records of 152 consecutive patients treated with SBRT from October 1999 through August 2005 were reviewed on an IRB-approved protocol. A total of 261 lesions in the lungs, liver, or other extracranial sites were treated; 18% (27/152) patients were treated on prospective Phase I/II studies. Ineligible patients or patients who declined to participate in the dose-escalation studies were treated with the highest safe dose established at the time of treatment (Fig. 1). Nearly all patients (97%) were treated in a 3 fraction course. Fig. 2. Characteristic fibrosis following high-dose SBRT to right lung metastatic lesion. Panel 1: Planning CT scan. Panels 2-6: 3,6,12,18,24 month follow-up scans, respectively. The patient has not recurred at time of analysis (36 months; image not shown). Fig. 3. Actuarial local control according to nominal dose. Lesions treated to a nominal dose of >54 Gy had a 3-year actuarial local control rate of 89.3%, whereas the values for those treated to 36-53.9 Gy and <36 Gy were 59.7% and 8.7% , respectively. The local control rate of treated tumors increased with escalated dose, expressed as either nominal dose or EUD. (Figure 3). Likewise, lesions treated with the highest third of EUD (>64.4 Gy) had a 3-year local control rate of 90.6%, compared to 56.0% in the middle third (43.5-64.4 Gy) and 9.9% in the lowest third (<43.5 Gy, p<0.0001). Figure 4. The highest dose given to a lesion near the proximal bronchial tree (see left 2 panels) was 54 Gy in 3 fractions. The patient did not experience pulmonary toxicity and remained locally controlled for 30 months before death from intercurrent illness. However, the patient did experience a Grade II vertebral fracture attributed partly to SBRT, although documented osteoporosis was a predisposing factor. Treatment was well tolerated; 3.4% of patients experienced grade 3 toxicity. Tumors near the proximal bronchial tree were generally treated to conservative doses (e.g. 36 Gy/3 fractions) following reports suggesting unacceptable toxicity associated with full-dose SBRT to that site. An example of an unusual skeletal event in such a case is shown in Figure 4. Conclusions This large single institution series suggests a dose-response relationship within the range of SBRT doses applied. Severe toxicity was uncommon. Excellent local control rates are achieved with a nominal (prescription) dose > 54 Gy in 3 fractions, corresponding to an EUD of >64.4 Gy. These results support the use of aggressive, high-dose SBRT regimens when durable tumor control is the primary objective. Figure 1: Date of treatment versus total nominal (prescribed) dose.