Download
1 / 56
690 likes | 1.15k Vues
Developments in the use of OSCEs to assess clinical competence. The Third International Conference on Medical Education in the Sudan. Katharine Boursicot, BSc, MBBS, MRCOG, MAHPE Reader in Medical Education Deputy Head of the Centre for Medical and Healthcare Education

E N D
Developments in the use of OSCEs to assess clinical competence The Third International Conference on Medical Education in the Sudan Katharine Boursicot, BSc, MBBS, MRCOG, MAHPE Reader in Medical Education Deputy Head of the Centre for Medical and Healthcare Education St George’s, University of London
Introduction of OSCEs Poor reliability: too small sample (1 or 2 cases); selection of cases random; examiner variation, unstructured marking • Why was the OSCE developed? • Dissatisfaction with traditional forms of assessing clinical competence • Long cases • Short cases • Vivas • Reliability and validity issues • Burgeoning field of medical education and psychometrics Poor reliability : too much variation in cases selected; same examiners followed candidate for all cases, unstructured marking Poor validity: tests knowledge, not clinical skills. Poor reliability: random content; examiner variation, unstructured marking
Characteristics of assessment instruments • Utility = • Reliability • Validity • Educational impact • Acceptability • Feasibility Reference Van derVleuten, C. The assessment of professional competence: developments,research and practical implications Advances in Health Science Education 1996, Vol 1: 41-67
Test characteristics • Utility = • Reliability • Validity • Educational impact • Acceptability • Feasibility • Reliability of a test/ measure • reproducibility of scores • capability of differentiating consistently between good and poor students
Reliability • Competencies are highlydomain-specific • Broad sampling is required to obtain adequate reliability • Need to sample candidate’s ability over several tasks • Need to have multiple observers
Blueprinting • Enables test to map to the curriculum outcomes • Allows sufficient sampling and specification of content (i.e. not random cases)
Number of assessors/observers per station • Is one good enough? • Wouldn’t two be better than one? • Why not have the assessor follow the candidate around the stations?
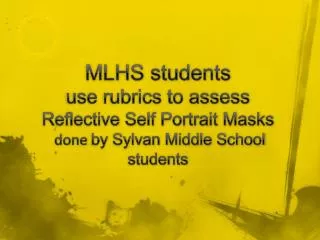
Reliability of scores on an OSCE 2 new examiners for each case 1 new examiner for each case Reliability Same examiner for each case Hours of Testing Time
Behaviour~ skills/attitudes Does Knowshow Cognition~ knowledge Knows Showshow Model of competence Professional authenticity Miller GE. The assessment of clinical skills/competence/performance. Academic Medicine (Supplement) 1990; 65: S63-S67.
Performance assessment in vivo: mini-CEX, DOPS, Video Does Performance assessment in vitro: OSCE, OSLER Knows how (Clinical) Context based tests: SBA, EMQ, SAQ Knows Factual tests: SBA -MCQ Shows how Testing formats Does Shows how Knows how Knows
Utility = • Reliability • Validity • Educational impact • Acceptability • Feasibility Test characteristics: Educational impact Relationship between assessment and learning Curriculum Assessment Teacher Student OSCE: encourages students to learn to perform the required skills
Advantages of using OSCEs in clinical assessment • Careful specification of content = Validity • Observation of wider sample of activities =Reliability • Structured interaction between examiner and student =Reliability • Structured marking schedule =Reliability • Each student has to perform the same tasks =Acceptability(fairer test of candidate’s clinical abilities)
Disadvantages of using OSCEs in clinical assessment – practical issues • Cost • Feasibility issues • Major organisational task • Requires many examiners to be present • Requires suitable facilities
Disadvantages of using OSCEs in clinical assessment – academic issues • In-vitro situation: testing competence, not testing actual performance in vivo with patients • Deconstruction of doctor-patient consultation into component parts – not holistic
Summary of reasons for use of OSCEs • OSCEs test clinical and communication skills - clinical competence • Reliable • Fair test for all candidates • Organisational and resource implications • Should be used as part of a programme of assessment
OSCEs • OSCEs have become very widespread • Undergraduate • Postgraduate • Medicine • Other clinical professions
Current issues • Problematic OSCEs • Authenticity • Standard setting • Compensation • SP recruitment, scripts and training • Examiner training
1. Problematic OSCEs Suboptimal practices which undermine the usefulness of using the OSCE format • Too few stations (less than 12) – poor reliability • Poorly blueprinted OSCE – insufficient spread of skills being tested - poor reliability and validity • MCQs/ SAQs/vivas disguised as OSCEs – poor validity • Poorly constructed stations (lack of congruence) - poor validity and reliability • Inconsistency in conduct of station (site, examiner, SP, equipment, timing) - poor reliability
2. Authenticity • Why should all stations last 5 minutes? • Not authentic • Some tasks require more time • Too little time = truncated ‘samples’ of clinical skills = NOT holistic • Match clinical situations as closely as possible • 5, 10, 15, 20 minutes
3. Standard setting • Process by which decisions are made about pass/fail • Wide variety of processes • Arbitrary • Overall judgement of examiner at each station • Angoff for each station • Complicated schemes involving grades • Gold standard method for OSCEs.......
Performance-based standard setting methods • These are the GOLD Standard for OSCEs • Borderline group method • Contrasting group method • Regression based standard method
1 2 3 4 5 Regression based standard Checklist X= passing score 1. Hs shjs sjnhss sjhs sjs sj 2. Ksks sksmsiqopql qlqmq q q qkl 3. Lalka kdm ddkk dlkl dlld 4. Keyw dd e r rrmt tmk 5. Jfjfk dd 6. Hskl;s skj sls ska ak akl ald 7. Hdhhddh shs ahhakk as TOTAL Checklist Score X Overall rating 1 2 3 4 5 Clear Borderline Clear Excellent Outstanding fail pass 1 = Clear fail 2 = Borderline 3 = Clear pass 4 = Excellent 5 = Outstanding
Performance-based standard setting • Advantages • Utilises the expertise of the examiners • they are observing the performance of the students • they are in a position to make a (global) judgement about the performance • based on • their clinical expertise • expected standards for the level of the test • knowledge of the curriculum/teaching
Performance-based standard setting • Advantages • Large number of examiners set a collective standard while observing the candidates – not just an academic exercise • Reliable: cut-off score based on large sample of judgments • Credible and defensible: based on expert judgment in direct observation
Performance-based standard setting • Disadvantages • Requires large (ish) cohort of candidates to achieve enough numbers in the ‘borderline’ group • Passing score not known in advance • Judgments may not be independent of checklist scoring • Requires expert processing of marks immediately after the exam • Checking of results • Delay in producing results
4. Compensation • A number of students achieve a totalscoreabove the overall pass markBUT • faila significant number of stations • Poor performance on a number of stations is compensated by good performance on other stations
Concerns • Students do not have an acceptable minimum standard across a range of skills • Students could proceed to graduation without having acceptable clinical examination or history taking skills
Criterion 2: Must pass ≥10/19 stations Two extra students failed Criterion 1: Pass mark 60.3 (BGM)


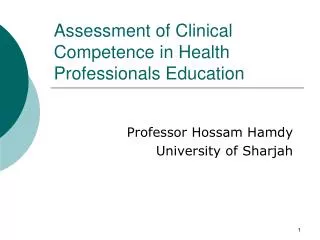
![LEVELS OF CLINICAL COMPETENCE [Cox, 1982]](https://cdn1.slideserve.com/1732043/levels-of-clinical-competence-cox-1982-dt.jpg)
![LEVELS OF CLINICAL COMPETENCE [Cox, 1982]](https://cdn1.slideserve.com/1732380/levels-of-clinical-competence-cox-1982-dt.jpg)