Download
1 / 19
190 likes | 624 Vues
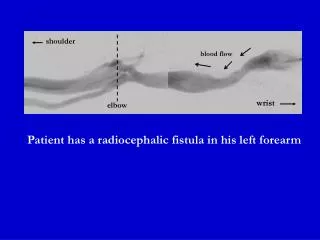
Fistula First: AV Fistula Maturation Project. Svetlana (Lana) Kacherova, QI Director Lisle Mukai, QI Coordinator ESRD Network 18 July 22, 2009. “Fistula First” GOAL. Goal is to maximize autogenous AVF construction & success rate…..

E N D
Fistula First: AV Fistula Maturation Project Svetlana (Lana) Kacherova, QI Director Lisle Mukai, QI Coordinator ESRD Network 18 July 22, 2009
“Fistula First” GOAL Goal is to maximize autogenous AVF construction & success rate….. To achieve in the shorter term (2006) the initial K/DOQI minimum benchmark of AVF use in 40% of prevalent patients…. And in the long-term (2009), a 66% AVF rate in prevalent patients Additional Goal: Reduce Catheter Use!
Fistula First Goals (AVF Rates) • CMS goal – 66% by June 30, 2009 • Yearly Network 18 goal – 57.8 % by June 30, 2010 • Yearly Network Stretch Goal – 58.0% by June 30, 2010 • May 2009 AVF rates: NW 18 – 56.3% US – 52.6%
Inclusion Criteria for Participating Facilities • AVF rate < 50% (April 08 SIMS data) • Highest percentage and number of AV Fistulas placed but not used (source: SIMS vascular access monthly reports) • Patients census > 50 patients • Administrative support: All intervention facilities have a stable leadership
Exclusion Criteria • Patient census < 50 patients • Facilities already included in another QIWP project with the Network
AVF Maturation Project:Network Role: • Project Leader • Supplied the templates for RCA & PDSA • Supplied toolkits to facilities & evaluate their usefulness • Provided monthly feedback (Vascular Access SIMS reports) • Collected bi-monthly scans to obtain facility-specific data • Facility site visits for strugglers • Chased facilities for data & documentation • Assisted participants to meet QAPI /PDSA requirements
Facilities Roles and Responsibilities: • Returned agreement letter (signed by MD) • Reviewed toolkit and identified tool(s) to utilize in your facility • Followed the project timelines and completing all steps of the QAPI process (RCA, PDSA, etc)
Project Timelines • Oct. 2008 – Environmental scan and WebEx • Nov. 208 – RCA and PDSA (steps 1-3) • Dec. 2008 – 1st follow-up • Jan-Feb. 2009 – 2nd follow- up • March-Apr. 2009 – 3rd follow up • May 2009 – final follow-up • June 2009 – Project summary and closure
Ensuring that Fistulas Mature The key is early recognition of non-maturing AVFs. • Physically assess the access each treatment (Look, Listen, Feel). • Send patient for 4 week follow-up evaluation of the access • Necessary intervention for non-maturing AVFs • Track all new AVFs and their development
Strategies Implemented by Facilities • Create Vascular Access Team (Interdisciplinary) • Designate Vascular Access Manager/ Coordinator • Educate staff and patients about what to look for and expect during AVF maturation process (physical assessment and vascular access care) • Refer to surgeon or Vascular Access Center for vein mapping
Schedule surgical appointment and 4 week follow-up • Obtain results of evaluation findings from the surgeon and maintain a copy in the patients charts as well as discuss during QAPI meetings • Track all newly placed AVFs and discuss/review during QAPI meetings • Physical exam (Look, Listen, & Feel) of AVFs every treatment by staff
Schedule follow-up evaluation for AVFs @ 4 weeks post placement of AVF • Track success rates from each vascular access surgeon – refer to surgeons with best results • Conduct stenosis monitoring & surveillance (See KDOQI Guidelines for appropriate surveillance methods.) • Create check-off list for each patient noting the steps of the plan
Monthly report of all new AVFs being cannulated – review during QAPI meetings • Utilize corporate vascular access tools (resources and tools) • Educate patients regarding catheters and fistulas (pros/cons) • Have MDs talk to patients about their vascular access and care for their access. • Involve SW for insurance issues
Next Steps • Have a process in place to ensure maturation of newly placed AVFs • Learn strategies from other facilities to implement at your facility if appropriate • Educate patients and their families, staff and nephrologists about the maturation process and vascular access care • Refer to the Fistula First website for resources
Next Steps (Continued) • Together we can make a difference and find possible solutions for issues we can impact Thank you for all your continuous efforts in improving vascular access care given to our ESRD population.
Svetlana (Lana) Kacherova, QI Director skacherova@nw18.esrd.net Lisle Mukai, QI Coordinator lmukai@nw18.esrd.net 6255 Sunset Boulevard Suite 2211 Los Angeles CA 90028 (323) 962-2020 (323) 962-2891/Fax www.esrdnetwork18.org