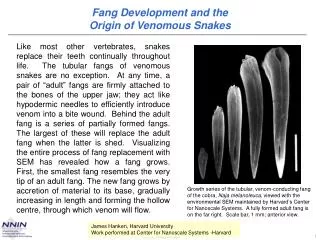
Venomous Snakebite
Venomous Snakebite. R Johnson MBBS MRCS DTM&H. Five Venomous Snake Families. Viperidae : N.American pit vipers (rattlesnakes, copperheads, mocassins), Asian pit vipers, African and Asian vipers and adders

Venomous Snakebite
E N D
Presentation Transcript
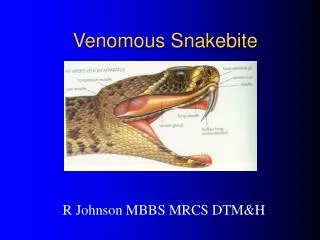
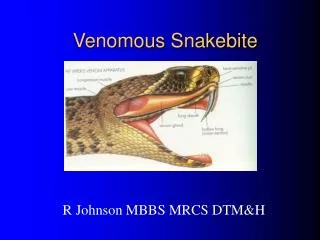
Venomous Snakebite R Johnson MBBS MRCS DTM&H
Five Venomous Snake Families • Viperidae: N.American pit vipers (rattlesnakes, copperheads, mocassins), Asian pit vipers, African and Asian vipers and adders • Elapidae: cobras, kraits, mambas, coral snakes, Laticauda seasnakes of Tropics, Sub-Tropics • Hydrophidae: seasnakes, Australasian venomous snakes • Colubridae: mostly non-venomous but includes rear-fanged boomslang, vine snakes, mole vipers, Japanese yamakagashi, Asian keelback • Actractaspididae: burrowing asps of Africa
Non-venomous python Elapid-mamba Pit viper Rear fanged boomslang Fang Types
Venomous snake behaviour • The majority of bites do not lead to envenomation • First bite is often a warning • Juvenile snakes more dangerous • Few snakes are aggressive; they are more scared of us • People to not drop dead in seconds!!! Many bites associated with alcohol or trying to tease or kill the snake 98% of U.S. snakebite due to pit vipers but exotic envenomations are becoming common as well Coral snakes seldom bite but can be very dangerous
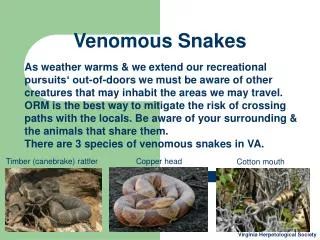
UK experience • One indigenous venomous snake • Vipera berus (adder) • 75-100 bites per year • Last fatality 1975 • Estimated 2000 dangerous snake “pets” • 15-20 bites per year • Most bites on the hand whilst picking up snake
Most dangerous U.S. snake Diamond Back Rattlesnake—a pit viper
Elapid Arizona Coral Snake Red touch yellow, kill a fellow; red touch black, fear may lack (in U.S.A.)
Red touch Black fear may lack only works north of Mexico City
Pit Vipers • Large thick-bodied snakes with triangular head • Heat–sensing pit • Elliptical pupils • Single row of scales past the anal plate • Rattle—if a rattlesnake! • Venom digests tissue and induces hemolysis and possible later kidney failure
Pit Viper N.A. Non-venomous
Two Venom Types: Hemolytic (Vipers)and Neurotoxic (Elapids) • Most Vipers and Pit vipers have a hemolyticor tissue-destroying digestive type of venom that causes immediate local pain and swelling (exceptions: some Mojave rattlesnakes are neurotoxic) • Most Elapids and Hydrophids (seasnakes) have a neurotoxic venom that produces little if any local symptoms—however cranial nerve palsies and respiratory arrest may follow (exception: spitting cobra bites will destroy tissue )
Pit Viper Venom • Enzyme cocktail: complex mixture of enzymes and small molecular weight peptides • Purpose is to immobilize and predigest prey, defense is secondary • Constituents: proteolytic enzymes, thrombin, collaginase, hyaluronidase, phospholipase A+B, crotamine (causes tetany), croactin, convulsin, gyroxin • 25% bites are dry + 25% minimal= 50% will be OK • Same antivenin used for all U.S. pit vipers: rattlesnakes, copperheads and cottonmouths
Swelling Pain: searing or burning Fang marks 1-4 Ecchymoses Vomiting Fasciculations Paresthesias Increased bleeding Blood blisters/blebs Lymphadenitis Metallic taste Arrhythmias Seizures Shock Coagulopathy (DIC) Thrombocytopenia Tetany Coma Death (usually takes days) Symptoms of Viper Envenomation
Measure Compartment Pressures but Never do prophylactic fasciotomy! Bad outcome often results
Check the Urine!!! Viper victims often survive the initial bite only to walk in and later die of renal failure Myoglobinuria due to tissue destruction can cause renal shutdown
Fatal Bite in a Toddler from Eastern Diamondback: Charleston, S.C.
First Aid in Snakebite • Calm and reassure victim • Remove rings, watches, tight clothes • Don’t catch or kill snake--second bite likely • Don’t cut fang marks or suck out with mouth • May use Sawyer-type venom extractor within 3m (leave on for 30m) • May use constriction band (no tourniquet) • Don’t use ice or electric shock • TRANSPORT ASAP TO HOSPITAL (phone and car keys most important emergency equipment) • Best not to administer antivenin in field setting!!!!! • No role for prophylactic antibiotics!
FBC with platelets Urinalysis ABG PT/PTT/fibrinogen (repeat w/in 12h) U&E/ creatinine Liver function tests Glucose ECG Type and Cross Creatinine kinase Snake Bite Investigations
Polyvalent Antivenin • Antivenin (Crotalidae) polyvalent: rattlesnake, copperhead, cottonmouth • Horse serum antibodies to venom; sheep (ovine) antivenin should be safer • Dangerous—give only under controlled situations where anaphalaxis can be managed • Expect serum sickness later; treat with prednisolone • If necessary, use enough (5+ vials for grade I, 5-15 for grade II, 15-20+ for grade III) • Dose not reduced for children! • Expensive: £200/vial
Antivenin Administration • Best w/in 4h but effective for at least 24h and possibly up to 72h with coagulopathy • Only give IV with physician in attendance and adrenaline and antihistamines available at bedside • If antivenin to be given, first skin test with horse serum kit unless pt in extremis. If (+) give only if true threat to life/limb and then pre-medicate with hydrocortisone IV and chlorphenaramine IV • If negative, still consider pre-medication w/ chlorphenaramine IV and Cimetidine 300 mg IV
Antivenin Administration • Reconstitute by injecting 10ml sterile water diluent to each vial and swirling (takes time) • Always get informed consent from pt or family if possible • Reconstituted antivenin vials are added to 500 ml NS or D5W then trial dose of 5-10 ml given over 5 minutes; epinephrine(1:1000) .3cc should be taped to IV bag just in case • If no reaction, adjust rate to give up to 10 vials in 1st hour w/ additional infusions every 2h until sign/sx resolving; common error: too little, too late • Fasciotomy rarely required with proper care
Serum Sickness • Expect 1-4 weeks after antivenin administration whatever the dose • Sx: itching, urticarial rash, fever, arthralgias • Rx: oral prednisolone therapy 60-80 mg with taper every 4 days • Many physicians anticipate serum sickness and discharge on steroids rather than waiting for it to develop
CroFab® Antivenin • Purified sheep antigen-binding fragment • Compared to equine IgG antivenom • More effective • Fewer and less severe adverse effects • No anaphylaxis reported to date • Currently approved only for rattlesnake bites • Cost $4600 to $14,000 (4 to 18 vials)
Contacts for help • Arizona Poison Control; 1-602-626-6016 • Good current source of information on exotic antivenin availability • Herpetologists available for consultation • Royal Veterinary College, London Tel: +44 (0)20 7468 5000 • Liverpool School of Tropical Medicine +44(0)151 705 3100 • Nearest zoo will keep antivenins for the snakes in its collection
Neurotoxic Envenomations • Elapids and Hydrophids—venom attacks nervous system and kills by respiratory arrest (hard to reverse) • Some snake venoms (e.g. cobra) are intermediate and are also hemotoxic causing severe local reactions like pit vipers • Minimal local reaction for most elapids (don’t wait for swelling to use antivenin!) • Rapid onset of neurologic symptoms: ptosis, respiratory paralysis, death • Fist Aid: immobilization and compression dressing • Swab wound for venom antigen ID (Australia) • Antivenin administration very soon
Red touch yellow, kill a fellow; red touch black, fear may lack Coral Snake (Micrurus) Bites • Elapid: bites rare since snake is secretive/shy • Local symptoms absent—systemic neurologic symptoms will develop first and will be difficult to reverse • Treat likely eastern coral bites with Micrurus antivenin immediately—bite is unimpressive • 3-5 vials if no signs or symptoms • 6-10+ vials if systemic symptoms exist
Large Constrictors can kill: never wrap a constrictor around your neck! Non-Poisonous Snakes can also kill
Snakebite Prevention • Wear protective clothing and boots • Avoid drugs and alcohol with snakes • Watch where you step and place your hands • Avoid tall brush and undergrowth • Leave snakes alone, don’t pick up dead snake or even a snake head (reflex bites) • Don’t keep venomous snakes as pets • Don’t walk after dark—if you do, use a flashlight
“Ha! Ain’t a rattler, Jake. You got one of them maraca players down your bag—and he’s probably more scared than you.”
Spider Bites/ scorpion stings • No native spiders of importance • Occasional pet spider bites • Most only mildly venomous • Treat like bee sting • Local measures; ice packs, analgesia and topical anaesthetic agents