Download
1 / 46
460 likes | 496 Vues
Explore guidelines for managing skin and soft tissue infections, including history, pathogenesis, definitions, etiologies, and prevention strategies for surgical site infections.

E N D
Soft tissue infections Guidlines for manegment of SSTIs Walid Elshazly Prof of surgery
Disclaimer • This presentation is based on a zero-fees contract with GSK; I did not receive any honoraria.
Community-Acquired Infections • SKIN AND SOFT TISSUE INFECTIONS • BREAST ABSCESS • PERIRECTAL ABSCESS • GAS GANGRENE • TETANUS • HAND INFECTIONS • FOOT INFECTIONS • BILIARY TRACT INFECTIONS • ACUTE PERITONITIS • VIRAL INFECTIONS
Hospital-Acquired Infections • PULMONARY INFECTIONS • UTI • WOUND INFECTIONS • INTRAABDOMINAL INFECTION • EMPYEMA • FOREIGN BODY-ASSOCIATED INFECTION • FUNGAL INFECTIONS • MULTIPLE ORGAN FAILURE
Skin and Soft Tissue Infection • Surgical site infections • Superficial infections • Impetigo • Erysipelas • Folliculitis • Furuncles and carbuncles • Hairadenitis supportiva • Superficial cellulites • Bites (animal or human) • Deep infections • Deep cellulites necrotizing form • Necrotizing fasciitis • Myo-necrosis • Gas gangrene • Streptococcal Toxic-Shock Syndrome
History • Soft tissue infections were first defined slightly more than a century ago. In 1883, Fournier described a gangrenous infection of the scrotum that continues to be associated with his name. • In 1924, Meleney documented the pathogenic role of streptococci in soft tissue infection. • Shortly thereafter, Brewer and Meleney described progressive polymicrobial postoperative infection of the muscular fascia with necrosis (the term necrotizing fasciitis was not introduced until the 1950’s). • The association between toxic-shock syndrome and streptococcal soft tissue infection was delineated as this disease reemerged in the 1980s.
Contact Dermatitis Necrotizing Fascitis Cellulitis Erysipelas Erythema Multiforme Ecthyma Deep Vein Thrombosis Folliculitis Impetigo
Definitions and Etiologies • Group of diseases that involve the skin and underlying subcutaneous tissue, fascia, or muscle. May be localized to a small area or may involve a large portion of the body. • May affect any part of the body, though the lower extremities, the perineum, and the abdominal wall are the most common sites of involvement. • Some are relatively harmless if treated promptly and adequately; others can be life-threatening even when appropriately treated.
Definitions and Etiologies • Symptoms and signs of SSIs • Pain (localized tendernes) loss of sensation • erythema, edema / induration • Blisters, crusted plaques • (Epi)dermal erosion and necrosis • Fluctuation, crepitus • Systemic signs of SIRS/Sepsis: • fever, tachycardia, hypotension, organ dysfuction
Definitions and Etiologies • Simple vs. complex • Primary vs. secondary vs. tertiary • Cellulitis vs. abscess • Superficial vs. deep • Necrotizing vs. non-necrotizing • Traumatic vs. non-traumatic • Dermatitis, fasciitis, myositis ( combinations) • Single vs. multiple pathogens • Classic syndromes: • Rapidly progressive infections • toxic shock syndromes • Specific etiologies or pathogens
Definitions and Etiologies • Non-traumatic - “Spontaneous” • Glandular infection (folliculitis, furuncle, carbuncle, hidradenitis, perianal-, perineal-, …) • Micro-trauma (cuts, insect bites, …) • Trauma (wounds - including surgical) • Clean Wounds: An uninfected operative wound in which no inflammation is encountered and the respiratory, alimentary, genital, or uninfected urinary tracts are not entered. • Clean-Contaminated Wounds: Operative wounds in which the respiratory, alimentary, genital, or urinary tracts are entered under controlled conditions and without unusual contamination. • Contaminated Wounds: Includes open, fresh, accidental wounds. In addition, operations with major breaks in sterile technique (e.g., open cardiac massage) or gross spillage from the gastrointestinal tract, and incisions in which acute, non-purulent inflammation is encountered are included in this category. • Dirty or Infected Wounds: Includes old traumatic wounds with retained or devitalized tissue and those that involve existing clinical infection or perforated viscera.
Surgical Site Infections • Factors that Increase Incidence of SSI • LOCAL 1.Wound Hematoma 2.Necrosis 3.Foreign Body 4.Obesity • SYSTEMIC 1.Age 2.Shock 3.DM 4.Malnutrition, Alcoholism 5.Immunotherapy 6.Steroids 7.Chemotherapy
Surgical Site Infections • SSI Prevention • Debridement, Irrigation, Bleeding control, Dirt and FB removal. • Preserve Oxygenation and Perfusion • Classification system of Wounds • Surgical Asepsis • Perioperative Antibiotics
Surgical Site Infections Surgical Asepsis • Clean wound infection is the Indicator of overall Sterile Technique in OR • Limit preoperative Hospitalization • Cleansing • Hair removal • OR time • Hemostasis, but beware of many sutures • Drains. Closed-suction, separate stab • Personnel, Respiration, Attire, Scrubbing, Gowns
Surgical Site InfectionsPerioperative Antibiotics- Prophylactic • Prophylactic antibiotics should exist at time of contamination. Clean- contaminated and Contaminated showed reduction • In clean only when Foreign Body is inserted • Preoperative, close to cutting time, long half- life, selected against specific pathogens, 4-6 hours later, and for 2 postoperative doses • Colon surgery: Oral antibiotics, poorly absorbed; neomycin- erythromycin along with mechanical preparation, and IV systemic • Dirty: fascial closure, wet-to-dry dressing and delayed primary closure in 4-5 days
Superficial infections • Impetigo • highly contagious, confined to the epidermis • usually face or extremities. • most common in infants and preschool children • dominant pathogen is S. aureus, less common S. pyogenes • skin lesions usually resolve spontaneously within 2 to 3 weeks. • antibiotic therapy accelerates the resolution
Superficial infections • Erysipelas • principally involves the dermis. infection extends through the dermal lymphatic vessels • tender, pruritic, intensely erythematous, hyperthermic, sharply demarcated, and raised plaque • most cases preceded by influenza like symptomspain (local, myalgia) , often high fever, and leukocytosis. • lymphangitis and -adenopathy sometimes present • lower leg most common site, followed by face, arms, and upper thighs. • almost invariably caused by S. pyogenes
Superficial infections • Erysipelas • antibiotic treatment • uncomplicated erysipelas: penicillin, cephs, amoxicillinare effective in at least 80% of cases. Oral and intravenous antibiotic regimens are equally efficacious. • patients with erysipelas of the lower extremity should be placed on bed rest, and the involved leg should be elevated • once the patient is able to resume normal activities, he or she should be fitted with elastic stockings, to help reduce the recurrence of edema and lower the risk of lymphedema. • For patients with tinea pedis, a topical antifungal agent is used to treat the infection and prevent recurrence.
Superficial infections • Folliculitis • infection of the hair follicle • painful, tender, erythematous papule with a central pustule single or multiple lesions in the skin of any hair-bearing area • typically caused by S. aureus. most resolve spontaneously within 7 to 10 days. • topical therapy: clindamycin, erythromycin, or mupirocin ointments chlorhexidine or benzoyl peroxide + warm soaks may accelerate resolution • with refractory or disseminated follicular infections:oral antibiotics S. aureus: dicloxacillin, erythromycin, cephalexin, cefadroxil, or clindamycin • Gram neg: oral ciprofloxacin; more aggressive therapy with systemic symptoms of sepsis
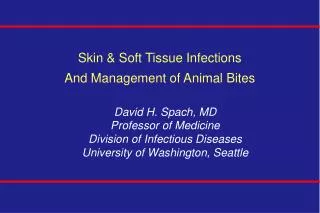
Carbuncle Furuncle, or boil
Superficial infections • Furuncle, or boil: small abscess • firm, tender, erythematous nodule • occurs in skin areas exposed to friction ( inner thighs and the axilla). also face, neck, upper back, and buttocks. • Initial treatment: • warm compresses to help promote drainage • oral antimicrobial agent effective against S. aureus • incision-and-drainage necessary when lesions do not drain spontaneously. Failure to drain these lesions adequately may result in recurrence, as well as in progression to a more serious infection.
Superficial infections • Carbuncle: deep cutaneous infection involving multiple hair follicles • characterized by destruction of fibrous tissue septa and formation of a series of interconnected abscesses. Patients commonly present with relatively large skin lesions (confluence) associated with chronic drainage, sinus tracts, and scarring • typically painful, red, tender, indurated area of skin with multiple sinus tracts. • Systemic manifestations (e.g., fever and malaise) are common. • occurs most frequently on nape of the neck, upper part of the back, or the posterior thigh. • Therapy: • incision-and-drainage w. thorough search for loculated areas should be undertaken • Wide local excision of the involved skin and subcutaneous fat is often necessary to prevent recurrent disease. • oral antistaphylococcal agent
Superficial infections • Cellulites • acute bacterial infection of the dermis and subcutaneous tissues • primarily lower extremities - can affect all other areas • Non-necrotizing Form = overwhelming majority • typically pain, soft tissue erythema, and constitutional symptoms (e.g., fever, chills, or malaise) • erythema with advancing borders, skin warmth, tenderness, edema. +/-Lymphangitis or -adenitis • usually single aerobic pathogen mostlyS. pyogenes and S. aureus
Superficial infections • Cellulitis • Therapy: empirical antibiotic regimen attempts to isolate pathogen are usually unsuccessful; • needle aspiration / skin biopsy at advancing margin positive < 15% / 40% • bacteremia is uncommon: blood cultures positive < 2% to 4% unless Sx of sepsis • In an otherwise healthy adult, uncomplicated cellulitis w/o systemic manifestations: oral antibiotic on an outpatient basis • majority of Strep and Staph are PCNase + cefadroxil ,amox/clav, cephalexin, dicloxacillin, erythromycin, or clindamycin • Diabetic or immunocompromised pts. and w. high fever or rapidly spreading cellulitis / cellulitis refractory to oral Abx (>48 h): admission for I.V. Abx. • Nafcillin, Cefazolin or ampicillin-sulbactam • Clindamycin for suspected MRSA and PCN allergies; Vancomycin, other Abx. and combination regimen
Superficial infections • Cellulitis • Necrotizing form: superficial vs. deep • “Superficial” necrotizing cellulitis • similar etiology and pathogenesis to nonnecrotizing cellulitis • Predominantly in PVD, diabetes, pressure ulcer, venostasis, lymphedema or neglected primary cellulitis • more serious and often progressive • pathogens similar + anaerobesclostridia, peptostreptococcus, bacteroides, … • Therapy: broad-spectrum Abx.urgent operative debridement is indicated+/- hyperbaric O2 therapy
Deep infections • Cellulitis • Necrotizing form: • Deep necrotizing cellulitis: (Necrotizing dermatitis, fasciitis, myositis) • extension of superficial infection or • primary deep space infection • crush / penetration / neglect / hematogenous • does not have to have skin necrosis • often lack of specific early signs & Sx, delayed diagnosis • most are polymicrobial • early: localized pain, tenderness, mild edema / erythema may be subtle -> cave: systemic illness > local signs • Later: bullae, intense erythema, skin necrosis, crepitus
Deep infections • Necrotizing form: • Deep necrotizing cellulitis: • Necrotizing fasciitis • angiothrombotic microbial invasion and liquefactive necrosis of deep subqutaneous tissues, fascia +/- muscle • Hallmark: dishwater tissue fluid, thrombosis of vesselsfrank necrosis occurs later initially, tissue invasion proceeds horizontally, • Myo-necrosis • rapidly progressive life-threatening infection • indicates involvement of Clostridium species. • short incubation: severe progressive disease in < 24 h • acute severe pain, often minimal physical findings • systemic signs of toxicity/ sepsis
Deep infections • Necrotizing form: • Deep necrotizing cellulitis: • Therapy: • broad-spectrum Abx to include MRSA, Gr.Neg and Clostridia bacteriocidal agents! • when clostridia suspected or confirmed, penicillin G, 2 to 4 million U every 4 hours immediately; clindamycin, 900 mg every 8 hours, should be added. • hyperbaric O2 therapy • operative debridement.
Deep infections Gas gangrene : is a bacterialinfection that produces gastissues in gangrene. It is a deadly form of gangrene usually caused by anaerobic bacteria. It is a medical emergency.
Streptococcal Toxic-Shock Syndrome • hemolytic streptococci of group A (S. Pyogenes) • more than 60% of patients with STSS have bacteremia. • current incidence 1.5 per 100,000 - STSS 10% to 15%, necrotizing fasciitis in 6%. • severe pain is the most common initial symptomsudden onset / generally precedes physical findings –> rapid progression. • hypotension invariably develops within 4 to 8 hours after presentation -> Shock, ,MOF, ARDS • Hemoglobinuria and an elevated serum creatinine, even w. adequate resuscitation
Streptococcal Toxic-Shock Syndrome • Clinical treatment failure sometimes w. penicillin alone attributable to the large inoculum size = Eagle effect • Clindamycin • more effective than b-lactam agents it suppresses bacterial toxin synthesis and inhibits M-protein synthesis, • Clindamycin also suppresses synthesis of penicillin-binding proteins, and it can act synergistically with penicillin.
Risk of infection 2-Infection agent : -Virulence -Numbers 1-Host : -Diet – vit.C . -Extreme age. -Chronic illness. -D.M, CLD, CRF -Medications: Steroid -Impaired immunity: HIV 3-Battle ground wound : -Ischemia -Necrosis -Gangreneous -Decrease WBC ,Abs
Risk of infection 2-Infection agent : -Virulence -Numbers 1-Host : -Diet – vit.C . -Extreme age. -Chronic illness. -D.M, CLD, CRF -Medications: Steroid -Impaired immunity: HIV 3-Battle ground wound : -Ischemia -Necrosis -Gangreneous -Decrease WBC ,Abs
Risk of infection 2-Infection agent : -Virulence -Numbers 1-Host : -Diet – vit.C . -Extreme age. -Chronic illness. -D.M, CLD, CRF -Medications: Steroid -Impaired immunity: HIV 3-Battle ground wound : -Ischemia -Necrosis -Gangreneous -Decrease WBC ,Abs
Risk of infection 2-Infection agent : -Virulence -Numbers 1-Host : -Diet – vit.C . -Extreme age. -Chronic illness. -D.M, CLD, CRF -Medications: Steroid -Impaired immunity: HIV 3-Battle ground wound : -Ischemia -Necrosis -Gangreneous -Decrease WBC ,Abs
Ceftriaxone (3r generation cephalosporin) SKIN AND SKIN STRUCTURE INFECTIONS caused by Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus pyogeneus, Viridans group streptococci, Escherichia coli, Enterobacter cloacae, Klebsiella oxytoca, Klebsiella pneumoniae, Proteus mirabilis, Morganella morganii,* Pseudomonas aeruginosa, Serratia marcescens, Acinetobacter calcoaceticus, Bacteroides fragilis* or Peptostreptococcus species. BACTERIAL SEPTICEMIAcaused by Staphylococcus aureus, Streptococcus pneumoniae, Escherichia coli, Haemophilus influenzae or Klebsiella pneumoniae.
Ceftriaxone (3r generation cephalosporin) SURGICAL PROPHYLAXIS: The preoperative administration of a single 1 gm dose of ceftroiaxone may reduce the incidence of postoperative infections in patients undergoing surgical procedures classified as • contaminated or • potentially contaminated