Download
1 / 34
370 likes | 627 Vues
Onyx use in embolization of CNS vascular lesions in pediatric patients. By Mohamed Nabil Hanafy Assistant lecturer – Department of Neurosurgery Menoufia university - Egypt. Introduction. Intracranial AVMs comprise 3 to 20 % of all AVMs

E N D
Onyx use in embolization of CNS vascular lesions in pediatric patients By Mohamed NabilHanafy Assistant lecturer – Department of Neurosurgery Menoufia university - Egypt
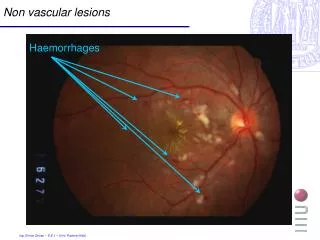
Introduction • Intracranial AVMs comprise 3 to 20 % of all AVMs • Spinal AVMs can present anytime during childhood. They often manifest as congestive or compressive myelopathy, back pain and less acutely as murmurs or pulsating para-spinal masses
30-50% of pediatric spontaneous ICH Morbidity rate: 50% Mortality rate: 5-10% for each hemorrhagic event Treatment is multidisciplinary Early treatment is recommended
Bristol and colleagues described the surgical treatment of 84 AVMs in 82 children, in this study >50% of patients received adjuvant therapy in the form of endovascular embolization or radiosurgery. The authors recommended the use of embolization as a preoperative therapy for grade II to IV lesions before surgery.
Embolization of AVMs is typically used to reduce nidal size prior to resection or radiosurgery. Improvements in embolization materials, catheters and techniques have made the "embolization for cure" an achievable target. In adult AVMs, the rate of complete endovascular obliteration is about 10% , although an exceptional 40% angiographic cure rate was reported by Valavanis and Yasargil.
Onyx Liquid Embolic Agent • Onyx (ev3 Neurovascular, Irvine, CA) was first described by Taki et al. and Terada et al. in the 1990s. From the chemical standpoint, it is an ethylene-vinyl alcohol copolymer (EVOH) dissolved in dimethylsulfoxide (DMSO). • It is a non-adhesive and radiolucent compound. Onyx-based closure of the lumen of the targeted vessel is obtained by means of precipitation, initiated after diffusion of DMSO in the presence of water. • These properties facilitate angiographic monitoring of embolization at any stage. Fluoroscopic visualization of the injected Onyx mass is possible through the addition of tantalum filings.
Onyx is supplied in ready-to-use vials. Each vial contains ethylene-vinyl alcohol copolymer, dimethylsulfoxide (DMSO), and tantalum. Ethylene-vinyl alcohol copolymer is formed of 48 mol/L ethylene and 52 mol/L vinyl alcohol. The polymer is dissolved in DMSO and is prepared in 3 different concentrations: 6.0%, 6.5%, and 8.0%. Micronized tantalum powder(35% wt/vol) is added for radiopacity. • The vials are kept on a shaker(Vortex-Genie, Scientific Industries, Bohemia, NY) for at least 20 minutes to ensure proper mixing of the tantalum powder. The lower the concentration of the copolymer, the less viscous the agent and the more distal penetration can be achieved.
The use of n-BCA in brain AVMs requires experience and skills, because intranidal flow and polymerization of n-BCA are quick and largely unpredictable. • The use of Onyx reversed the traditional “inject and run” approach adopted with acrylic glue is replaced by the need and possibility for slow progressive injection lasting several minutes. • Onyx 18 and Onyx 34 have been approved by the Food and Drug Administration (FDA)in July 2005 for the pre-surgical embolization of brain AVMs in adults. The use of Onyx in pediatric patients is still off-label. • The safety and efficacy of the use of Onyx in embolization of CNS arteriovenous lesions in pediatric patients aren't well studied.
Germanwala et al. reported on a 1 year old child with a residual vein of Galen malformation who had been treated with coils via trans-arterial and trans-venous routes at the age of 20 days, subsequently embolized to closure by using Onyx 18. * GermanwalaAV, Vora NA, Thomas AJ, Jovin T, Gologorsky Y, Horowitz MB: Ethylenevinylalcohol copolymer (Onyx-18) used in endovascular treatment of vein of Galen malformation. Childs NervSyst 24:135–138, 2008
Eddleman et al.described 2 cases of infectious intracranial aneurysms, one of them was treated totally and uneventfully with Onyx 18, and the other one was partly obliterated with coils then Onyx 18 was used for complete obliteration. In the second case distal Onyx migration happened but didn't result in any neurologic deficits. * EddlemanCS, Surdell D, DiPatri A Jr, Tomita T, Shaibani A: Infectious intracranial aneurysms in the pediatric population: endovascular treatment with Onyx. Childs NervSyst 24: 909–915, 2008
Jankowitz et al. reported on 21 procedures done on 6 patients to treat 8 lesions. 4 patients had brain AVMs (one of the patients had 3 AVMs) and 2 patients had VOGMs. Onyx was used alone to obliterate 3 lesions, while coils and embospheres were used before Onyx in the rest of cases. The procedures were complicated by transient neurological changes in 1 patient with brain AVM and death in the 2 patients with VOGMs within 24 hours of embolization due to intracranial hemorrhage.
Thiex et al. presented the first large series of Onyx embolization in CNS AV lesions in children. • The report included 15 pediatric patients who underwent 36 transarterialembolizations by using Onyx for CNS AV lesions.
Underlying pathologies included brain AV malformations(AVMs) (n = 7), vein of Galen malformations (n = 4), dural AV fistulas (n = 2), and spinal AVMs (n = 2). For 7 procedures in very high-flow lesions, detachable coils were deployed before Onyx embolization, whereas in 29 procedures, Onyx was the sole embolic agent. • Embolization was complete in 2 patients, nearly complete in 9 patients, and partial in 4 patients. Following staged embolization, 7 patients underwent surgical resection without significant blood loss and with good functional outcome in all cases. • Clinically silent non-target embolization was encountered in 2 of 36 procedures. After 3 of the 36 embolizations, patients developed transient neurologic symptoms, all of which resolved to baseline within 24 hours. • The study reported no vessel perforation, vessel dissection, unintended vessel occlusion, or stuck catheters. There were no post-embolization hemorrhages or territorial infarcts. There was neither permanent neurologic morbidity nor mortality.
Regarding the techniques of embolization, Thiex et al. preferred staged embolization and described the "stacking technique" where Onyx 34 was first slowly injected by using rapid gentle taps under fluoroscopic guidance, with pauses of 15 seconds to 2 minutes to create a plug around the microcatheter tip, providing the equivalent of a wedged microcatheter position. Care was taken not to allow significant reflux of Onyx up the microcatheter tip (<10 mm in a straight vessel, and <5 mm in a tortuous vessel of small caliber). In most not purely fistulous cases, the Onyx 34 syringe was then exchanged for the Onyx 18, to allow better penetration of nidal vessels. In purely fistulous cases, Onyx34 was used throughout. • In 7 cases of high-flow AV fistulas or purely fistulous component of a mixed lesion, platinum coils (Guglielmi detachable coil, BostonScientific; or Axium; ev3) were deployed as close to the point of AV shunt as possible, to reduce rapid inflow into the vein. After coil deployment, Onyx could be injected with excellent flow control, permeating through the coil mass to the shunt point. • Regarding follow up rules, an immediate postoperative angiogram was obtained when embolization was followed by surgical resection. Follow-up angiography was scheduled 6 months following definitive treatment.
Soltanolkotabi et al. managed to puplish a larger series of Onyx embolization in CNS AV lesions in pediatric patients. Twenty-five patients (mean age 10.5 years) underwent a total of 38 procedures. An aggregate of 56pedicles were embolized (mean 1.47 per session).Complete obliteration of the AVM in 3 cases (12%) and partial obliteration in 22 cases (88%). A total of 23 patients underwent surgical treatment. The mean preoperative AVM devascularization in these cases was 72%. One patient was treated with radiosurgery following Onyx embolization. Overall, 10 complications occurred in a total of 38 procedures (26.3%). None of the complications resulted in permanent neurological morbidity.
The rate of transient neurological complications was 10.5% (4 of 38 procedures) and the rate of transient non-neurological complications was 5.3% (2 of 38 procedures). The remaining 4 complications were clinically silent (rate of 10.5%). • There were no procedure-related deaths in this study population. • There was no significant difference in patients with and without complications in terms of demographic characteristics, AVM grade, or embolization features (p ≥ 0.2).Deep venous drainage was associated with higher complication rates (p = 0.03).
Ashour et al. described 105 endovascular procedures on 69 patients with heterogeneous group of vascular disorders and tumors. The group included 52 patients(75%) with primary vascular lesions: • 34 cerebral AVMs • 6 VOGMs • 4 DAVFs • 3 Spinal AVFs • 3 Head and neck AVMs • 2 Mycoticcerebral aneurysms 17 patients (25%) with hypervasculartumors: • 9 juvenile nasal angiofibromas (JNAs) • 3 spinal aneurysmal bone cysts • 1 cerebellarMB • 1 cerebellarhemangioblastoma • 1 supratentorialGBM • 1 scalp hemangioma • 1 sacral giant cell tumor
The mean number of procedures per patient was 1.52 (range, 1-6). Mean number of pedicles embolized per procedure was 1.7 (range, 0-6).Coils were used adjunctively in 20 (19%), n-BCA in 17 (16%), and polyvinyl alcohol particles in 2 (2%) procedures. • The author described complications in 25 of 105 total procedures (23.8%), of which 9 (8.6%)were clinically silent, 14 (13.3%)produced transient deficits, and 2 (1.9%) produced permanent deficits. • No significant differences found between those who did and those who did not experience complications in terms of age, sex, mean pedicles embolized, mean estimated AVM devascularization, Spetzler-Martin AVM grade, AVM pretreatment Rankin Scale score, use of coils/n-BCA, or institution at which the embolization was performed. No procedure-related deaths were reported; however, 2 deaths occurred remotely after and were unrelated to embolization.
Fifty-one embolization procedures were done for 34 cerebral AVMs, of which 4 cases (11.7%) were totally obliterated by embolization alone, and 24 cases (71%) underwent post-procedural complete surgical excision. Of the remaining 6 AVMs, 1 was partially embolized and subsequently treated with Gamma Knife radiosurgery, and 5 were partially obliterated after embolization and either are being followed up or further treatments are planned. Fifteen procedures (29.4%) had complications in the form of: • 3 non-target cerebral artery-to-artery embolizations • 2 microcatheter-related vessel perforations • 2 intracerebralhemorrhages • 2 episodes of focal cerebral edema • 2 episodes of DMSO-induced pulmonary edema • 1 embolization territory infarct • 1 nontargetcerebral-to-pulmonary-artery embolization • 1 retained microcatheter • 1 episode of contrast-induced bronchospasm. • Five complications (9.8%) were clinically silent, 9 (17.6%)produced transient deficits, and 1 (2.0%) produced a permanent deficit.
Six VOGMs underwent 15 embolization procedures. Four cases are being followed up clinically with known residual lesions. One case had total obliteration and another case had near total obliteration. Complications happened in 6 of 15 procedures (40%) in the form of 3 small embolization territory infarcts, 1 IVH requiring temporary ventriculostomy, 1 non-target cerebral-to-pulmonary-artery embolization, and 1 retained microcatheter, and none had permanent deficits. • Three out of 4 DAVF cases had total obliteration using both transarterial and transvenous routes. Two mycotic cerebral aneurysms were completely occluded with Onyx, but one of them had permanent neurological morbidity resulting from postembolization ischemia in the territory of the arterial branch from which the mycotic aneurysm arose.
The extracranial vascular lesions included uneventful embolization for 2 patients with masticator space AVMs and 1 patient with a forehead AVM. Three patients had spinal AVFs; there was1 case of epidural AVF and 1 case of type IV perimedullary AVF, 2both completely obliterated with Onyx. The third patient had 2 type IV perimedullary AVFs: 1 completely obliterated by Onyx embolization alone and 1 surgically resected without endovascular treatment.
Eighteen tumor embolizations were carried out in 17 patients with an 85% mean post-procedural devascularization. • Four JNA cases were embolized directly via an endoscopic endonasal puncture ; the remaining14 embolizations (78%) were performed via a standard trans-femoral approach. • Complications occurred in 2 of 18 tumor embolization procedures (11.1%): 1 transient episode of facial ischemia after JNA embolization and 1 clinically silent microcatheter-related vessel perforation during cerebellar MB embolization. There were no permanent complications.
The complication rate approximating 1 in 4 cases is somewhat alarming, although few long-term deficits were appreciated. This may serve as commentary on the plasticity of the pediatric brain rather than the severity of the complications. • Despite the big number of patients in this study, the study has some limitations: • Diverse pathological entities studied • Different approaches (in some tumors endoscopic direct puncture and injection was used) • Potential differences in treatment style between the 2 participating institutions • Retrospective nature • Lack of control groups • Restricted follow-up
Squid (Emboflu, Switzerland) is a new EVOH copolymer that has been introduced to clinical practice recently with 4 different formulations (18, 18LD, 12 and 12LD.)The LD versions have 30% less tantalum which may help visualize structures behind dense embolic casts under X ray. The micronized tantalum particles in Squid are smaller than Onyx and allegedly provide a more homogeneous solution. Squid offers less viscous formulation (Squid 12)for improved vascular penetration and as a lower density formulation (Squid LD) compared to Onyx. • Akmangit et al. reported on 28 patients (16 AVMs, 9 AV fistulas, 2 tumors and 1 AICA aneurysm) who were treated with Squid 18 and Squid 12.
Complication avoidance • Microcatheter-Related Vessel Perforation • DMSO-compatible catheters required for Onyx embolization are stiffer and less flexible at the tip and require a microwire for navigation • The tortuous anatomy and small dysplastic feeding vessels in pediatric patients • Choose safer pedicles • Avoid forceful injection of Onyx or contrast
Microcatheter entrapment • The FDA declared that neither Onyx nor the catheter is intended be a long-term implant, and patients may need additional medical interventions to have the catheter removed if it becomes entrapped. • Since Jan. 1, 2005, the FDA has received more than 100 reported cases, including nine patient deaths, of catheter breakage that may be related to catheter entrapment. • In some cases the catheter could be removed. In at least 54 of these cases, it was not possible to remove the catheter. • In April 2012, the FDA approved changes to the physician and patient labeling that reflect the risks related to catheter entrapment. • Leaving the catheter is safer than forceful extraction trials • Maintain anticoagulation therapy
Non-target Embolization • cerebral artery-to-artery / cerebral artery–to–pulmonary artery • Injected Onyx within the catheterized vessel exits the microcatheter tip in the shape of a “string” rather than a “ball,” making visualization of the Onyx difficult despite roadmap imaging, allowing unrecognized transit through the venous system into the pulmonary artery. • avoid early occlusion of the venous drainage • Control the depth and speed of penetration by using the stacking technique or the plug and push technique, or you can use coils before onyx to slow the flow
Hemorrhagic Complications • FDA Onyx/n-BCA equivalence trial, 1 hemorrhage (rate of 2%) and 1 stroke (rate of 2%), both causing permanent deficits, were reported in 54 adult AVM patients that underwent preoperative Onyx embolization. • Staged embolization is preferred by most of the authors specially when hemodynamic instability is expected • Be cautious in the final stages of complete embolization when the risk of compromising the venous outflow is greatest.
DMSO-related toxicity • The reported average dose during FDA trials leading to approval of Onyx for cerebral AVMs was 205 mg/kg • DMSO toxicity is more common in children compared with adults • Avoid fast injections • Be cautious in the presence of arteriovenous shunting • Staged embolization for large lesions
Radiation exposure • total patient radiation exposure may be related in part to the longer injection times and the ability to perform multiple intra-procedural angiographic runs when Onyx is used. • The topic isn’t well studied • No specific effort to minimize radiation exposure was mentioned in any of the studies
Conclusion • The available reports on the use of Onyx in pediatric neurointerventions assume that Onyx can be used effectively for embolization of pediatric cranial and spinal vascular lesions and tumors with low permanent morbidity • Future prospective controlled trials are needed with more specification of the pathological entities under treatment