
Abstract
Choriocarcinoma in a Viable Term Pregnancy Complicated by Subarachnoid Hemorrhage and Preeclampsia: A Case Report Dr Stephane M. Foulem, Dr Cherry Pike Memorial University, Department of Obstetrics and Gynecology, St John’s, Newfoundland, Canada. Case Presentation

Abstract
E N D
Presentation Transcript
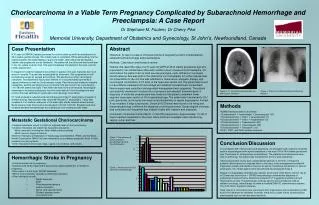
Choriocarcinoma in a Viable Term Pregnancy Complicated by Subarachnoid Hemorrhage and Preeclampsia: A Case Report Dr Stephane M. Foulem, Dr Cherry Pike Memorial University, Department of Obstetrics and Gynecology, St John’s, Newfoundland, Canada Case Presentation A 31 year old G6P3A2 female presented for routine follow-up with her obstetricians at 35+5 weeks gestational age. She initially had no complaints. While descending from the examining table she noted feeling a “pop in her head”, after which she developed a sudden and progressive frontal headache. The patient left the office and was found later in her car unable to drive home. She was immediately transferred to the case room for further assessment. In triage she noted the headache was similar in quality to her past migraines but much worse in severity. The pain was exacerbated by movement. She complained of both photophobia as well as nausea and vomiting. She denied any further neurological symptoms. Past obstetrical history was relevant for 3 uncomplicated spontaneous vaginal deliveries as well as 2 first trimester losses. Past history was limited to migraine headaches, asthma and carpal tunnel syndrome. She was found to be normotensive (110/78) with stable vital signs. Fetal heart rate was found to be reactive. Neurological examination (including fundoscopy) found no focal deficits. Initial investigations were normal. She was admitted for observation and neurology consultation. CT head revealed a subarachnoid hemorrhage and initial CT angiography revealed no evident etiology. Neurosurgery was consulted.Repeat CT angiography 7 days later revealed a 2 cm fusiform aneurysm of the distal right middle cerebral arterial branch. Blood pressure was then found to be elevated (120/100-140/102). Repeat blood work revealed elevated transaminases and a diagnosis of preeclampsia was made. Abstract Objective: To report a case of choriocarcinoma in pregnancy at term complicated by subarachnoid hemorrhage and preeclampsia Methods: Case report and literature review Results: We report the case of a 31 year old G6P3 at 35+5 weeks gestational age who presented to her obstetricians office with sudden onset of severe frontal headache. On examination the patient had no focal neurological signs, neck stiffness or increased blood pressure. She was sent to the obstetrical unit immediately for further assessment. On presentation to the unit she was admitted for observation, analgesic therapy and neurological consultation. A CT scan of the head was carried out. The patient was found to have diffuse subarachnoid hemorrhage with bilateral intraventricular involvement. Neurosurgery was consulted and expectant management was suggested. The patient subsequently developed increased blood pressure and elevated transaminases. A diagnosis of moderate preeclampsia was made and the patient underwent lower segment caesarean section at 36+6 gestational age. The patient was transferred to ICU post-operatively and lung lesions were noted incidentally on repeat angiography. A chest X-ray revealed 6 large lung lesions. Serum β-hCG levels were found to be rising and placental pathology confirmed the diagnosis of choriocarcinoma. Gynecological oncology was consulted and the patient was treated initially with cisplatin and etoposide. Conclusion: Choriocarcinoma affects 1 in 50,000 pregnancies. Approximately 1 in 30 of these reported metastasis to the brain. More common metastatic sites include lung, vagina, vulva, and liver. Figure 3: CT Head Demonstrating Blood in both Lateral Ventricles Figure 4: Chest X-ray Showing Several Pulmonary Nodules • Methods • PubMed literature search (all articles): • “Subarachnoid” + “hemorrhage” + “preeclampsia” (37) • “Choriocarcinoma” + “brain” + “preeclampsia” (1) • “Choriocarcinoma” + “brain” + “hypertension” (2) • “Choriocarcinoma” + “hypertension” (48) • “Choriocarcinoma” + “preeclampsia” (95) • “Choriocarcinoma” + “aneurysm” (33) • SOGC, FIGO, and WHO website searches. • Metastatic Gestational Choriocarcinoma • Cerebral metastasis occurs in 3-28% of reported cases of choriocarcinoma. • Cerebral metastasis can present as neoplastic aneurysms. • Most commonly involving the distal middle cerebral arteries • Most common shape is fusiform • Both the International Federation of Gynecology and Obstetrics (FIGO) and the World Health Organization (WHO) list brain metastasis as an adverse prognostic factor in their respective scoring systems. • Other metastatic sites include lungs, vagina, liver, kidneys, and ovaries. Figure 1: Overall serum β-human chorionic gonadotropin (β-hCG) Trend Postpartum Conclusion/Discussion In consultation with neurosurgery and anesthesia, an emergent lower segment Cesarean section was arranged under spinal anesthesia in the main OR at 36+6 weeks gestational age. There were no intraoperative complications. The placenta and membranes were sent for pathology. The patient was transferred to the ICU post-operatively. Initial postoperative course was complicated by delirium in the form of visual and auditory hallucinations that resolved within a few days. Initial management included IV magnesium sulfate and labetolol infusions as well as nimodipine and dilantin for seizure prophylaxis. All of these agents were discontinued by postoperative day 3. Repeat CT angiography revealed lung masses, which were confirmed on chest x-ray. β-hCG level was found to be > 100’000 and pathology confirmed the diagnosis of gestational choriocarcinoma. Abdominal and pelvic CT suggested possible liver and renal lesions as well. The gynecology oncology service was consulted as well as radiation oncology. Initial therapy included a modified EMA/CE chemotherapy regimen. The child had no apparent sequelae. Case reports of choriocarcinoma occurring in term pregnancies and complicated by SAH exist in the literature we reviewed. However, there are no cases further complicated by preeclampsia such as we have described here. • Hemorrhagic Stroke in Pregnancy • 5-fold increased rate in pregnancy. • Subarachnoid hemorrhage (SAH) accounts for approximately 3% of strokes in pregnancy. • SAH occurs in 2.4-4.3 per 100’000 deliveries. • SAH is most commonly caused by underlying aneurysm. • Other etiologies include: • Septic aneurysm • AVM • Preeclampsia/eclampsia • Arterial dissection • Spinal cord vascular lesion • Pituitary apoplexy/lesion • Chorocarcinoma Figure 2: Recent serum β-hCG Trend Post-Chemotherapy


















