Neuroblastoma
720 likes | 1.29k Vues
Neuroblastoma. Neuroblastoma. A tumor of postganglionic sympathetic neuroblasts The sympathetic chain extends from the neck to the sacrum The adrenal gland Neurotransmitter- Catecholamines. Neuroblastoma - Epidemiology. Most common extracranial solid tumor Incidence – 10/million per year

Neuroblastoma
E N D
Presentation Transcript
Neuroblastoma A tumor of postganglionic sympathetic neuroblasts The sympathetic chain extends from the neck to the sacrum The adrenal gland Neurotransmitter- Catecholamines
Neuroblastoma - Epidemiology • Most common extracranial solid tumor • Incidence – 10/million per year • ~10% of pediatric tumors • Peak age – 2-3 years • >90% cases before 5 years • Mostly sporadic – rare genetic associations • Most common neonatal tumor
Neuroblastoma - Genetics Mostly sporadic – rare (2%) genetic associations (NF1, Hirschsprung, congenital central hypoventilation syndrome) Mutations in ALK (tyrosine kinase) Environment??
Neuroblastoma – Biology • Neuroblastoma is a tumor of undifferentiated (embryonal) neuroectodermal cells, derived from the neural crest • An aberration of normal differentiation • An abnormal response to normal neurotropic signals (TRK-A, NGF) • Spontaneous regression • Differentiation – Ganglioneuroma, ganglioneuroblastoma
Neuroblastoma – Clinical features I • Tumor originates from sympathetic ganglia/adrenal gland • Lymphatic and hematogenous spread • Metastases to bone, liver, bone marrow, skin • Most patients present with advanced disease (40% of all patients, 55% of patients over 1 year)
Neuroblastoma-Clinical features - II Abdominal mass (65%) Thoracic mass (Infants) Bone pain Fever Weight loss “Sick looking child”
Neuroblastoma – Clinical Features - III • Lower limb paresis – 20 to spinal epidural tumor (4%) • Severe diarrhea 20 to secretion of VIP (vasoactive intestinal peptide) (4%) • Horner syndrome - patients with cervical or upper thoracic sympathetic ganglia (1.7%) • Hypertension, flushing, sweating (0.2%) • Raccoon eyes • Pallor, bleeding diathesis (Bone marrow involvement)
Neuroblastoma Raccoon eyes
Neuroblastoma – Clinical features - IV Opsoclonus-Myoclonus syndrome Acute cerebellar encephalopathy characterized by cerebellar ataxia, rapid and random eye movements (opsoclonus) and myoclonic jerks (2.8%) Good oncological but poor neurological outcome
Laboratory Features • Catecholamines (Dopamine, epinephrine, VMA, HVA) • Serum markers - LDH, ferritin, NSE (Neuron specific enolase) • Blood count (BM involvement) • Coagulation (Liver involvement)
Pathology • Small round blue cell tumor • Neuroblastic differentiation: From very undifferentiated to differentiated • Degree of anaplasia – Shimada index • Biological parameters
Neuroblastoma biology II • N-MYC – Oncogene on chromosome 2 amplification – worse prognosis • DI (DNA Index= ploidy) – hyperdiploid – better outcome in infants • 1p deletion – putative tumor suppressor genes – worse prognosis • 17q gain – oncogene?
N-Myc amplification • Amplification – A localized genomic change that results in increased dosage of a gene or genes affected • Homogeneously staining regions (HSR’s) - are areas on the native chromosome with multiple 100-200 kB copies of the region containing the amplified gene • Double minutes (DM) – Extrachromosomal fragments containing the amplified gene • >10 copies are associated with a worse prognosis
Neuroblastoma - Staging • CT/MRI • MIBG (Meta-iodo-benzyl-guanidine) • Bone scan • Bone marrow aspirate and biopsy • Surgery
Neuroblastoma - INSS Staging System Stage 1- Localized tumor with complete gross excision, with or without microscopic residual disease; representative ipsilateral lymph nodes negative for tumor microscopically (nodes attached to and removed with the primary tumor may be positive) Stage 2A – Localized tumor with incomplete gross resection; representative ipsilateral non-adherent lymph nodes negative for tumor microscopically Stage 2B- Localized tumor with or without complete gross excision, with ipsilateral non-adherent lymph nodes positive for tumor’ enlarged contralateral lymph nodes must be negative microscopically Stage 3 – Unresectable unilateral tumor infiltrating across the midline, with or without regional lymph node involvement; or localized unilateral tumor with contralateral regional lymph node involvement; or midline tumor with bilateral extension by infiltration (unresectable) or by lymph node involvement Stage 4 – Any primary tumor with dissemination to distant lymph nodes, bone, bone marrow, liver, skin, and/or other organs (except as defined for stage 4s) Stage 4s – Localized primary tumor (as defined for stage 1, 2A or 2B) with dissemination limited skin, liver, and or bone marrow (limited to infants<1 year)
2b 4 1 2a 3 4S International Neuroblastoma Staging System (INSS)
Prognostic Factors Age (<18m – favorable) Stage Histology (Shimada) Biology N-MYC, DI, 17q+, 1p-
Neuroblastoma - Treatment Risk adapted Low risk NB – Minimal therapy – excellent outcome High NB – Intensive therapy – poor outcome
INRG – International Neuroblastoma Risk Group Classification System Age Stage N-MYC status
Low/Intermediate risk Neuroblastoma Watch and wait (No treatment=no toxicity) Surgery- Minimize damage Low intensity chemotherapy Radiation – emergency only (rarely used)
Improving Survival for Stage 4 Neuroblastoma Patients > 1 Year of Age at Diagnosis 1 0.8 Childrens Cancer Group Data Probability of Overall Survival 0.6 0.4 1986-1995 N = 675 0.2 1978-1985 N = 507 P < 0.001 0 1 2 3 4 5 6 7 8 9 10 Years from Diagnosis
Treatment – High Risk Neuroblastoma Induction chemotherapy Surgery High dose chemotherapy with stem cell rescue (Eradication of residual disease) Radiation Retinoic Acid Immunotherapy
High-risk Neuroblastoma – Treatment Roadmap ████████████ ██ ██ Induction Surgery Consolidation XRT Cis-RA Immunorx. Chemotherapy ABMTAnti GD2 IL-2 GM-CSF (Differentiation therapy) Immunotherapy
Chemotherapy in Neuroblastoma Platinum (Cis, carbo) VP-16 Doxorubicin Cyclophosphamide/Ifosfamide Vincristine Topotecan
High Dose Chemotherapy Myeloablative doses Eradication of tumor Rescue with autologous stem cells MEC (Melphalan, etoposide, carboplatinum) BM (Busulfan, Melphalan)
Neuroblastoma – Radiation Therapy • Local consolidation (In high-risk disease) • Massive hepatomegaly in infants with 4S • Cord compression? • Metastatic disease - palliation
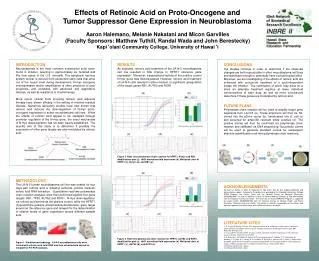
Neuroblastoma – Differentiation therapy • Cis-retinoic acid (Roaccutane) • Induces differentiation of neuroblastoma cells in vitro and decreases proliferative capacity • Shown in randomized clinical trial to improve outcome
High-Dose, Pulse Retinoic Acid Induces Neuroblastoma Differentiation Control 10 mM Retinoic Acid
Neuroblastoma – Immunotherapy Anti GD-2 antibodies Interleukin 2 GM-CSF
Accrual of 386 randomized patients needed
COG-ANBL0032 Phase III 2/17/09 Status: DATA AND SAFETY MONITORING COMMITTEE With ~61 % of accrual in, and ~ 2 year median follow up, the Immunotherapy arm shows: Superior EFS (p = 0.0115) Superior OS (p = 0.0223)