Unexplained Chronic Cough
Unexplained Chronic Cough. Dr Surinder Birring Consultant Respiratory Physician Honorary Senior Lecturer King’s College Hospital & King’s College London London. Outline. Case study Impact on QOL Unexplained cough Non-pharmacological therapy. Why is cough important?.

Unexplained Chronic Cough
E N D
Presentation Transcript
Unexplained Chronic Cough Dr Surinder Birring Consultant Respiratory Physician Honorary Senior Lecturer King’s College Hospital & King’s College London London
Outline • Case study • Impact on QOL • Unexplained cough • Non-pharmacological therapy
Why is cough important? • Most common reason to consult GP • Antitussive drug sales USA >$4billion/yr • Chronic cough (>8wk): 12% population • 10-38% of out-patients referrals
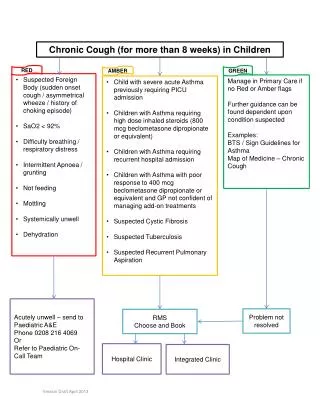
Causes of chronic cough • Lung cancer • COPD • TB • Fibrosis • Heart failure • Sarcoidosis • Foreign body • Abnormal: • Examination • CXR • Spirometry
Case study • 64 year old lady • Seen by 3 respiratory consultants • Referred to cough clinic by GP • Tickly dry cough 2003 • Post nasal drip • Reflux • Never smoked
Investigations • CXR/CT normal • FEV1 normal Post Nasal Drip • ENT review/nasal steroid/antihistamine Asthma • Oral / inhaled corticosteroids GOR • 3month+ omeprazole • 24-hr oes pH study -ve
Unexplained chronic cough • Idiopathic cough • Refractory cough • Persistent cough • Psychogenic cough • Tic cough • Sensory neuropathic cough
Is she coughing? 24 Hour cough monitor: LCM Hidden Markov Models Ambulatory Single coughs Automated 24 Hours Birring et al, ERJ 2008; 31:1013-1018
Adverse impact of chronic cough Worried about serious illness 77% Concerned something is wrong 72% Frequent nausea 56% Exhaustion 54% Others think something is wrong with me 53% Embarrassment 49% Self-consciousness 46% Difficulty speaking on the telephone 39% Urine incontinence 30% Absence from work 11% French C et al, Arch Intern Med 1998; 158:1657
Depressive symptoms in chronic cough 60 50 40 CES-D Score > 16 (%) 30 20 10 0 IHD Asthma Heart Failure Diabetes Chronic cough Severe COPD Hypertension Dicpinigaitis P et al, Chest 2006; 130:1839
Anxiety: HAD and STAI scores Mc Garvey L et al, Cough 2006; 2:4
QOL questionnaires COUGH Birring S et al, Thorax 2003; 58:339-343 KBILD ILD Patel A et al, Thorax 2012; 67:804 SARCOIDOSIS Patel A et al, Thorax 2012; In press KSQ
Physical Chest pains Sputum Tired Paints/fumes Sleep Frequency Hoarse Voice Energy Psychological Embarrassed Anxious In control Frustrated Fed up Serious illness Other people Social Conversation Annoy family Job Enjoyment HRQOL: The LCQ Birring S et al, Thorax 2003; 58:339-343
Cough frequency & QOL 100 80 Cough frequency c/hr 60 40 r = -0.6 20 0 4 6 8 10 12 14 16 18 20 LCQ scores Birring et al, Resp Med 2006; 100:1105-9
Gender differences in QOL * 5.5 * 5 4.5 MALES LCQ SCORE FEMALES 4 *p<0.05 3.5 3 PHYSICAL PSYCHOLOGICAL SOCIAL Birring et al, ATS 2003
Cough Intensity Oesophageal pressure Flow rate Abdominal EMG activity Cough sound
Female patients cough harder during max voluntary cough Thoracic pressure Cough flow
Cough Sound Explosive Voiced Intermediate
Cough Sound: a novel objective marker of intensity? Energy Maximum frequency
Unexplained cough or cause yet to be identified? Enlarged tonsils Birring et al, Eur Resp J 2004; 23: 199-201
Birring et al, Thorax 2003;58:533-6 Birring et al, Thorax 2003;58:1066-70 Birring et al, Resp Med 2004; 98: 242-6 Birring et al. Thorax 2005;60:249-253
Unexplained cough: prevalence Most recent reports: 40% Morice et al, ERJ 2004; 24:481-92
Unexplained cough: profile Female 70% Onset around menopause Cough duration, many >5 years Poor QOL High levels anxiety, depressive and obsessive traits
Mrs X: Treatment options for unexplained cough • Amitriptyline • Gabapentin • Morphine • Physiotherapy/Speech therapy
Gabapentin: randomised controlled trial p=0.012 Full Treatment Period Ryan N et al, Lancet 2012:380:1583
Cough Suppression Physiotherapy • Education (avoid triggers, no benefit of excessive cough) • Laryngeal hygiene (reduce alcohol/caffeine, sips water, avoid mouth breathing, correct abnormal breathing pattern+ VCD) • Cough control (chew sweets, forced swallow, huff, distraction) • Counselling (reinforcement of techniques, modify behaviour, address adverse symptoms such as incontinence) Patel A et al; Chronic Resp Dis 2011;8:253-8
Psychology and the cough clinic • As part of our clinical physiotherapy cough suppression service stress and anxiety is covered for our chronic cough patients • Booklet was designed by Dr Hutton, Helene Bellas and Sarah Chamberlain for chronic cough patients to cover stress and anxiety and how it affects their cough. Which covers: • The general affects cough has on the body • How anxiety can make cough worse as patients are: • Less likely to identify their cough triggers • Less likely to remember and implement the cough suppression techniques they have been taught • Affects their breathing pattern • If patients are anxious about coughing they tend to over focus on coughing
Chest physiotherapy for refractory chronic cough n=23 *p=0.003 *p<0.001 *p=0.03 7 6 5 Before 4 After LCQ Domain Score 3 2 1 0 Physical Psychological Social Patel A et al; Chronic Resp Dis 2011;8:253-8
T1 T2 T3 T4 Screen VAS QOL CM CRS VASQOL VAS QOL VAS QOLCM CRS VAS QOL(post) VAS QOL(post) PSALTI Trial Placebo Observation Screen Physiotherapy Randomisation DAY -7 0 7 14 28 56 84 Treatment
Summary • Chronic cough is a common • Frequently unexplained • High physical and mental health morbidity • Few drug treatment options • Integrated physical and mental health approach needed • Future research -illness perception/behaviour -Early detection of mental health problems -Develop cough specific behavioural therapies -Increase awareness of psychological morbidity
Acknowledgements King’s College Kai Lee Sarah Chamberlain Rachel Harding Rachel Garrod Jane Hutton Aish Sinha Jonathan La-Crette Amit Patel Helene Bellas Alka Savani John Moxham Irene Higginson Gerrard Rafferty Tracey Fleming Claire Woods Lynne Morgan Collaborators Ian Pavord Sergio Matos David Evans Gillian Watkins Ben Prudon Debbie Parker Fan Chung Alvin Ing Kevin Chan Nicole Ryan Peter Gibson